15 December 2025: Articles 
Compartment Syndrome Secondary to Phlegmasia Cerulea Dolens in a Patient With Crohn’s Disease
Unusual clinical course, Challenging differential diagnosis, Management of emergency care, Rare coexistence of disease or pathology
Saad Mohammed AlshahraniDOI: 10.12659/AJCR.948950
Am J Case Rep 2025; 26:e948950






Abstract
BACKGROUND: Phlegmasia cerulea dolens is a rare, potentially fatal complication of deep vein thrombosis characterized by sudden limb swelling, pain, and cyanosis. The prevalence of venous thromboembolism is estimated to be 1.5 to 3.5 times higher in patients with inflammatory bowel disease than in the general population. Without prompt treatment, it may progress to venous gangrene, compartment syndrome, or circulatory shock. Crohn’s disease, a chronic inflammatory bowel disorder, increases the risk of thromboembolic events due to persistent inflammation and hypercoagulability, which can precipitate phlegmasia cerulea dolens.
CASE REPORT: A 26-year-old male smoker with a history of fistulizing Crohn’s disease, nonadherence to his prescribed regimen, chronic pulmonary embolism, and prior inferior vena cava filter placement presented with acute right lower limb swelling and pain. Doppler ultrasonography revealed extensive iliofemoral deep vein thrombosis extending into the inferior vena cava; clinical evaluation confirmed compartment syndrome. Emergency fasciotomy and popliteal artery embolectomy restored circulation and prevented ischemic injury. Subsequently, the patient required a blood transfusion due to lower gastrointestinal bleeding, followed by an emergent exploratory laparotomy with right hemicolectomy, ileocecal resection, and ileostomy after colonoscopy failed to identify an active bleeding source. The patient recovered well postoperatively.
CONCLUSIONS: This case highlights the importance of early recognition and prompt management of phlegmasia cerulea dolens in patients with inflammatory bowel disease, particularly among younger individuals with an increased risk of thrombotic complications.
Keywords: Compartment Syndromes, Crohn Disease, fasciotomy, Thrombosis, Humans, Male, adult, Thrombophlebitis, Venous Thrombosis
Introduction
Phlegmasia cerulea dolens (PCD) is a rare, life-threatening manifestation of deep venous thrombosis that presents with sudden, extensive limb swelling, pain, and cyanosis, typically due to obstruction of the iliofemoral veins. Without timely treatment, PCD may progress to venous gangrene, compartment syndrome, or circulatory shock, highlighting the importance of early intervention [1]. Risk factors include malignancy, hypercoagulable states, and venous stasis [2]. PCD typically affects the left leg and is more common in older women [3]. Due to its rarity, contemporary large-scale epidemiologic data are limited; most available evidence are derived from older case series and retrospective analyses. Nevertheless, PCD remains a high-risk condition: venous gangrene develops in approximately 40% to 60% of cases, and mortality rates range from 20% to 40% [4]. These outcomes highlight the need for prompt recognition and aggressive management.
Crohn’s disease, a form of chronic inflammatory bowel disease (IBD), is associated with an elevated risk of thromboembolic events due to chronic inflammation and hypercoagulability [5]. The prevalence of venous thromboembolism (VTE) in patients with IBD is estimated to be 1.5 to 3.5 times higher than that in the general population [6]. A long-term, population-based study in Manitoba, Canada showed that the overall incidence of VTE among individuals with IBD was 7.6%, compared with 3.3% among controls. Specifically, individuals with Crohn’s disease demonstrated an incidence of 8.4%, compared with 6.9% among individuals with ulcerative colitis [7]. Similarly, in a prospective cohort study of 149 patients with IBD, 5% of those with Crohn’s disease had a documented history of thromboembolic events, including deep vein thrombosis (DVT), stroke, myocardial infarction, and pulmonary embolism (PE), further illustrating the clinical relevance of this risk [8]. The mechanisms underlying the increased risk of VTE among individuals with IBD remain incompletely understood but appear multifactorial, involving dysregulation of the coagulation cascade, endothelial dysfunction, platelet activation, and impaired fibrinolysis. The chronic inflammatory state in Crohn’s disease alters both coagulation pathways and endothelial integrity, predisposing patients to events such as DVT and, in rare instances, PCD [6]. Prompt diagnosis and intervention are essential to prevent irreversible ischemic damage in patients with PCD. Therapeutic options include anticoagulation, thrombolysis, and surgical thrombectomy; fasciotomy is sometimes required in cases complicated by compartment syndrome [9]. This case report describes a rare instance of PCD in a young patient with Crohn’s disease that progressed to lower limb compartment syndrome and PE, emphasizing the importance of vigilance for thrombotic complications in this population.
Case Report
A 26-year-old male smoker with a history of fistulizing Crohn’s disease diagnosed 8 years earlier presented with poor adherence to his prescribed medication regimen, which included azathioprine 50 mg orally once daily and infliximab 5 mg/kg intravenously each month. His medical history also included right pneumothorax secondary to right middle lobe cystic changes and empyema, which had been managed with a right middle lobectomy, as well as chronic recurrent PE for which an inferior vena cava (IVC) filter had been placed. The patient had initially been treated with apixaban when right segmental PE was diagnosed; after an instance of pneumothorax complicated by empyema and considering his ongoing nonadherence to anticoagulation, the decision was made to insert an IVC filter. During the present case, the patient attended the emergency department with a 1-day history of progressive swelling in the right lower limb, accompanied by pain and restricted range of motion. He reported decreased oral intake of solids and liquids, poor appetite, reduced activity, dizziness, and increased bloody diarrhea over the preceding 5 days.
On examination, the patient was hypotensive, with a blood pressure of 88/56 mmHg, and tachycardic, with a heart rate of 121 beats/min. Other vital signs were unremarkable, including a respiratory rate of 17 breaths/min, oxygen saturation of 100%, and temperature of 36.3°C. His body mass index was 14.5 kg/m2, with a height of 178 cm and weight of 46 kg. He received a 30 mL/kg bolus of intravenous normal saline, which improved his blood pressure. His remaining vital signs were stable. The right leg was diffusely swollen from the inguinal region to the foot, pale, and mottled with bluish discoloration (Figure 1). Femoral pulses were palpable, and the right popliteal pulse was weakly palpable. In contrast, the posterior tibial and dorsalis pedis pulses were not palpable. The patient was unable to flex or extend his toes; he demonstrated no dorsiflexion or plantarflexion of the ankle against gravity. However, minimal movement was observed when gravity was eliminated, corresponding to a grade of 2/5 on the Medical Research Council Scale for Muscle Strength. Sensation in the affected limb was diminished.
Bedside and Doppler ultrasonography revealed substantial DVT in the iliofemoral vein. The Doppler study demonstrated triphasic waveforms in the femoral and popliteal arteries, monophasic waveforms in the posterior tibial artery, absence of detectable waves in the dorsalis pedis artery, and positive venous signals, indicating impaired arterial circulation and venous involvement. A continuous infusion of sodium heparin at 1000 U/mL was initiated, with subsequent prothrombin time and partial thromboplastin time values of 12.20 s and 34.20 s, respectively. Run-off computed tomography angiography revealed progressive non-opacification of the right infrageniculate arteries with distal loss of opacification; however, no distinct truncation or arterial embolus was identified in the right lower limb (Figure 2).
Pelvic computed tomography demonstrated extensive right lower limb venous thrombosis extending above the IVC filter into the infrahepatic IVC. The thrombosis was accompanied by asymmetrical soft tissue enlargement and congestion in the right thigh (Figure 3), prompting clinical evaluation for possible compartment syndrome. A diagnosis of acute right lower limb compartment syndrome secondary to extensive iliofemoral DVT and ischemia was established. Computed tomography venography to further assess thrombus extension was deferred to prevent delays in surgical management. Vascular surgery was consulted urgently. After computed tomography angiography confirmation of non-opacification of the right infrageniculate arteries, the patient underwent emergency fasciotomy using a double-incision technique and popliteal artery embolectomy. Blood flow was successfully restored; small thrombi were removed from the anterior and posterior tibial arteries. Leg color and tissue perfusion rapidly improved, and good biphasic Doppler signals were obtained. The patient tolerated the procedure well and was transferred to the intensive care unit for close observation. Shortly thereafter, he developed lower gastrointestinal bleeding. Emergent colonoscopy revealed no active bleeding site. Computed tomography angiography of the lower gastrointestinal tract demonstrated no evidence of active contrast extravasation or bleeding; thus, embolization was not performed. After appropriate resuscitation with blood transfusion, general surgery was consulted. The patient underwent emergent exploratory laparotomy with right hemicolectomy, ileocecal resection, and ileostomy. He remained in the intensive care unit for 7 days before transfer to the Gastroenterology ward. The patient was eventually discharged on low-molecular-weight heparin 40 mg twice daily and scheduled for IVC filter removal. He was ambulatory at discharge after a total hospital stay of 40 days.
Discussion
PCD is a rare but severe complication of DVT that may progress to compartment syndrome requiring urgent intervention [10]. Compartment syndrome is usually diagnosed using a Stryker needle and comprises compartment pressure measurements of 30 mmHg or greater (normal pressures are typically below 10 mmHg); alternatively, it is regarded as a compartment pressure within 30 mmHg of the diastolic blood pressure [11]. The pathophysiology of compartment syndrome in PCD involves venous hypertension secondary to obstruction of venous outflow, leading to interstitial edema and substantial fluid accumulation within the affected limb. This accumulation contributes to third-space fluid loss, which can precipitate hypovolemic shock. As compartment pressure rises, it may exceed arterial wall tension, causing arterial collapse. Subsequent elevation of interstitial and compartment pressures results in acute ischemia and venous gangrene, considerably increasing morbidity and mortality [12]. Within 6 h, compartment pressures may rise by up to 16-fold due to severely impaired venous drainage [10]. Although a few cases have been documented in the literature [10–14], compartment syndrome secondary to PCD remains rare. These reported cases matched the presentation of our patient, who exhibited classic features of PCD, including extensive swelling, cyanosis, and loss of motor and sensory function in the affected limb. The rapid progression of these symptoms, coupled with diminished distal pulses and imaging that confirmed extensive iliofemoral DVT with impaired arterial flow, was consistent with the expected pathophysiology. The urgent need for fasciotomy and embolectomy reflected the critical nature of compartment syndrome in this setting and highlighted the importance of early recognition and timely surgical intervention in improving patient outcomes in such rare cases.
Intriguingly, younger patients with IBD have a greater likelihood of developing VTE relative to individuals without the condition. A nationwide Danish study demonstrated that both the incidence and relative risk of VTE unrelated to surgery, trauma, or pregnancy were higher among younger patients with IBD, especially those aged 20 years or younger, indicating a strong association between early-onset IBD and thrombotic risk [15]. This finding aligns with the clinical history of our 26-year-old male patient with fistulizing Crohn’s disease, who experienced recurrent VTE episodes, including chronic PE, despite IVC filter placement. His poor adherence to immunosuppressive therapy and recent disease flare with bloody diarrhea likely further increased his thrombotic risk. Recurrent VTE in patients with IBD has also been shown to occur more frequently after cessation of anticoagulation, as demonstrated in the present case. A 2010 cohort study comparing patients with and without IBD who had a first unprovoked VTE episode revealed that the 5-year recurrence rate after discontinuing anticoagulation was significantly higher in the IBD group. Notably, younger age at the time of the initial thrombotic event was independently associated with an increased risk of recurrence, emphasizing the importance of early risk stratification and consideration of extended anticoagulation in this population [15]. The recurrence of thrombosis after prior discontinuation of anticoagulation in our patient further supports findings in the literature, suggesting that prolonged or indefinite anticoagulation is warranted for young patients with IBD exhibiting high-risk profiles.
Patients with PCD usually present with blue or purple discoloration of the affected limb, accompanied by swelling, pain, and, in severe cases, loss of pulses [16]. Because of the anatomical relationship in which the right iliac artery crosses over the left iliac vein, most cases involve the lower extremities; the left leg is more frequently affected than the right [12]. However, our patient presented with right lower limb ischemia secondary to extensive iliofemoral DVT. Gong et al evaluated the association between the location of lower extremity DVT and PE. They found that right-sided DVT was a more frequent cause of PE than left-sided DVT, consistent with our patient’s history of chronic PE [17]. Endothelial wall damage can occur through various mechanisms. Direct causes include mechanical disruption during procedures such as catheter insertion [18]. Notably, our patient had undergone IVC filter placement, which was intended to prevent recurrent PE due to his history of chronic embolic disease. As highlighted in prior studies, the present case underscores the delicate balance between the preventive role of IVC filters and their potential to increase VTE risk, making close monitoring essential [19]. Indirect endothelial wall damage may occur through inflammatory mechanisms [18]. In our case, the patient’s Crohn’s disease, a form of IBD, further increased his risk of thrombosis. IBD enhances the likelihood of VTE by approximately 1.5 to 3.5 times and is associated with considerable morbidity and mortality [20,21]. Endothelial dysfunction is a central feature of IBD pathogenesis, characterized by an imbalance between vasodilatory and vasoconstrictive mediators, typically driven by inflammation [22]. This imbalance alters the structural and functional properties of endothelial cells [23]. The resulting prothrombotic state in IBD increases susceptibility to severe thrombotic complications such as PCD, as demonstrated in the present case [24]. Our patient demonstrated malnutrition, as reflected by his low body mass index. In severe IBD, particularly ulcerative colitis, malnutrition and nutrient deficiencies can impair coagulation factor synthesis, thereby predisposing patients to VTE [25].
Endovascular therapies such as percutaneous mechanical thrombectomy and catheter-directed thrombolysis, as well as surgical intervention, may be considered treatment options. However, these approaches carry risks, including periprocedural PE and venous endothelial injury [26]. The severity of ischemia determines whether an endovascular or surgical approach is most appropriate [27]. In the present case, the patient underwent emergency fasciotomy combined with popliteal artery embolectomy. The decision to perform fasciotomy was driven by the need for rapid decompression of elevated compartment pressure, which, if not promptly managed, can result in irreversible ischemic damage to the affected tissues [28]. Embolectomy addressed the arterial occlusion via direct removal of thrombi from the popliteal artery, restoring blood flow by means of an invasive but definitive procedure.
Conclusions
PCD with compartment syndrome is rare but associated with high morbidity and mortality among patients with IBD, particularly younger individuals who exhibit an increased risk of VTE due to chronic inflammation and coagulation abnormalities. This risk is driven by chronic systemic inflammation, dysregulation of the coagulation cascade, endothelial dysfunction, platelet activation, and impaired fibrinolysis. Right-sided DVT, as demonstrated in the present case, may further enhance the risk of PE. Prompt recognition and aggressive management are essential to restore venous flow, prevent limb loss, and address the added complication of compartment syndrome, which requires urgent decompression and close monitoring.
Figures
 Figure 1. Right lower limb swelling and blue discoloration.
Figure 1. Right lower limb swelling and blue discoloration. 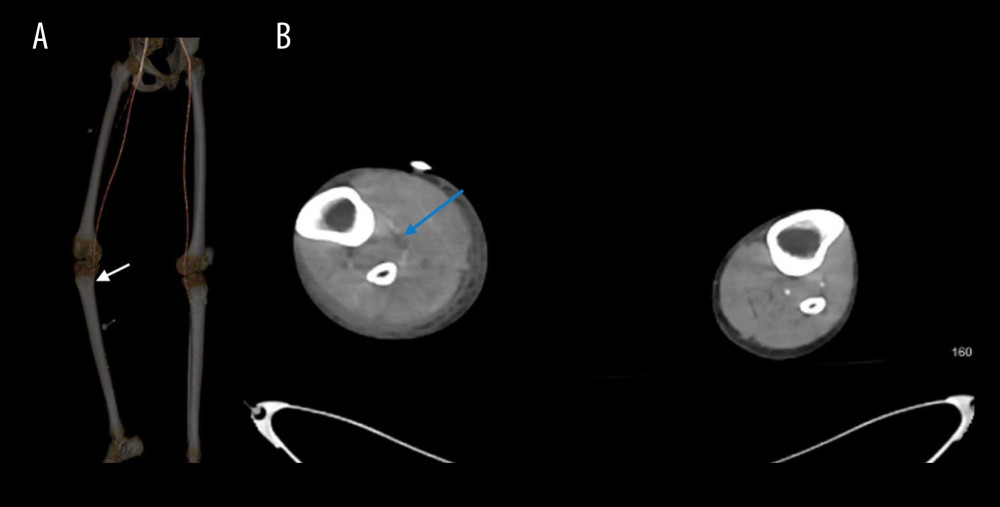 Figure 2. Computed tomography imaging demonstrating progressive non-opacification of the right infrageniculate arteries. (A) Lower limb computed tomography angiography revealing progressive non-opacification of the right infrageniculate arteries with distal loss of opacification (white arrow). (B) Abdominopelvic computed tomography (cross-sectional view) showing progressive non-opacification of the right infrageniculate arteries (blue arrow).
Figure 2. Computed tomography imaging demonstrating progressive non-opacification of the right infrageniculate arteries. (A) Lower limb computed tomography angiography revealing progressive non-opacification of the right infrageniculate arteries with distal loss of opacification (white arrow). (B) Abdominopelvic computed tomography (cross-sectional view) showing progressive non-opacification of the right infrageniculate arteries (blue arrow). 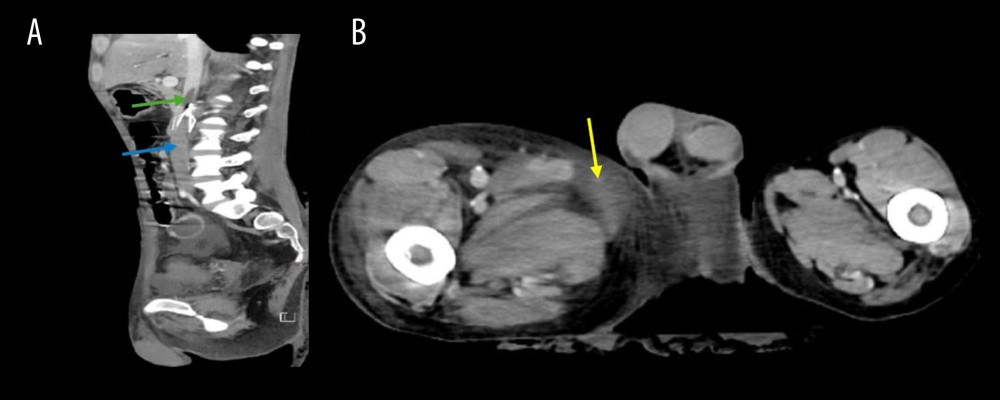 Figure 3. Abdominopelvic computed tomography imaging demonstrating venous thrombosis and associated soft tissue changes. (A) Abdominopelvic computed tomography (sagittal view) showing venous thrombosis extending above the inferior vena cava (IVC) filter (green arrow) into the infrahepatic segment (blue arrow). The IVC filter is visible immediately below the green arrow but not separately labeled. (B) Abdominopelvic computed tomography (cross-sectional view) showing asymmetrical soft tissue enlargement and congestion in the right thigh (yellow arrow).
Figure 3. Abdominopelvic computed tomography imaging demonstrating venous thrombosis and associated soft tissue changes. (A) Abdominopelvic computed tomography (sagittal view) showing venous thrombosis extending above the inferior vena cava (IVC) filter (green arrow) into the infrahepatic segment (blue arrow). The IVC filter is visible immediately below the green arrow but not separately labeled. (B) Abdominopelvic computed tomography (cross-sectional view) showing asymmetrical soft tissue enlargement and congestion in the right thigh (yellow arrow). References
1. Ogeng’o JA, Ongera D, Sinkeet SR, Phlegmasia cerulea dolens: A review of pathophysiology and management strategies: Int J Vasc Med, 2021; 2021; 7809435
2. Hussain MA, Aljabri B, Al-Omran M, The importance of recognizing phlegmasia cerulea dolens in patients with high-risk conditions: J Vasc Surg Venous Lymphat Disord, 2018; 6(1); 32-39
3. Chinsakchai K, Ten Duis K, Moll FL, Phlegmasia cerulea dolens: Incidence and outcomes in older adults: Eur J Vasc Endovasc Surg, 2020; 59(2); 335-42
4. Klok FA, Huisman MV, Seeking optimal treatment for phlegmasia cerulea dolens: Thromb Res, 2013; 131(4); 372-73
5. Koutroubakis IE, Tsiolakidou G, Koumoutsos I, Risk of thrombosis in inflammatory bowel disease: A comprehensive review: World J Gastroenterol, 2015; 21(3); 793-802
6. Cheng K, Faye AS, Venous thromboembolism in inflammatory bowel disease: World J Gastroenterol, 2020; 26(12); 1231-41
7. Bernstein CN, Nugent Z, Singh H, Persistently high rate of venous thromboembolic disease in inflammatory bowel disease: A population-based study: Am J Gastroenterol, 2021; 116(7); 1476-84
8. Carvalho AC, Pinho J, Cancela E, Inflammatory bowel disease and thromboembolic events: A clot to learn: Ther Adv Gastroenterol, 2022; 15; 17562848221100626
9. Hozumi J, Hozumi T, Takahashi Y, Emergency management of phlegmasia cerulea dolens with compartment syndrome: A case report: Am J Emerg Med, 2019; 37(12); 2276e5-e8
10. Aydemir B, Hoyle C, Hakmeh W, Phlegmasia cerulea dolens causing compartment syndrome: Am J Emerg Med, 2022; 61; 234e1-e3
11. Davidson AL, Sutherland MA, Siska RC, Janis JE, Practical review on the contemporary diagnosis and management of compartment syndrome: Plast Reconstr Surg Glob Open, 2024; 12(3); e5637
12. Gardella L, Faulk JB, Phlegmasia alba and cerulea dolens [Updated 2022 Oct 3]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK563137/
13. Chaochankit W, Akaraborworn O, Phlegmasia cerulea dolens with compartment syndrome: Ann Vasc Dis, 2018; 11(3); 355-57
14. Dah K, Ogbu IR, Ngwudike C, Tripathi M, Right lower extremity phlegmasia cerulea dolens due to iliotibial vein thrombosis with compartment syndrome and circulatory shock: Case report and review: Cureus, 2022; 14(12); e32364
15. Coremans L, Strubbe B, Peeters H, Venous thromboembolism in patients with inflammatory bowel disease: Review of literature and practical algorithms: Acta Gastroenterol Belg, 2021; 84(1); 79-85
16. Zhang Q, Yang L, Chang L, Analysis and literature review of deep vein thrombosis related phlegmasia cerulea dolens diagnosis in critically patients: Case Rep Clin Med, 2023; 12(8); 312-23
17. Gong S, Lee EJ, Kim JS, Association between laterality and location of deep vein thrombosis of lower extremity and pulmonary embolism: Vasc Specialist Int, 2021; 37; 12
18. Ashorobi D, Ameer MA, Fernandez R, Thrombosis [Updated 2024 Feb 12]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK538430/
19. Grewal S, Chamarthy MR, Kalva SP, Complications of inferior vena cava filters: Cardiovasc Diagn Ther, 2016; 6(6); 632-41
20. Chung WS, Lin CL, Hsu WH, Kao CH, Inflammatory bowel disease increases the risks of deep vein thrombosis and pulmonary embolism in the hospitalized patients: A nationwide cohort study: Thromb Res, 2015; 135(3); 492-96
21. Kohoutova D, Moravkova P, Kruzliak P, Bures J, Thromboembolic complications in inflammatory bowel disease: J Thromb Thrombolysis, 2015; 39(4); 489-98
22. Cibor D, Domagala-Rodacka R, Rodacki T, Endothelial dysfunction in inflammatory bowel diseases: Pathogenesis, assessment and implications: World J Gastroenterol, 2016; 22(3); 1067-77
23. Boussi L, Safaya A, Goyal A, “Inflammatory bowel disease – not just the bowel’s bane”: Peripheral arterial and venous thrombosis in a patient with Crohn disease: Vasc Endovascular Surg”, 2020; 54(7); 646-49
24. Zezos P, Kouklakis G, Saibil F, Inflammatory bowel disease and thromboembolism: World J Gastroenterol, 2014; 20(38); 13863-78
25. Cryer B, The risks of deep vein thrombosis in patients with ulcerative colitis and COVID-19: Proc (Bayl Univ Med Cent), 2024; 37(2); 248-49
26. Šimon S, Roman S, Case report of simultaneous phlegmasia cerulea dolens and acute limb ischemia: Int J Surg Case Rep, 2024; 125; 110596
27. Kou CJ, Batzlaff C, Bezzant ML, Sjulin T, Phlegmasia cerulea dolens: A life-threatening manifestation of deep vein thrombosis: Cureus, 2020; 12(6); e8587
28. Torlincasi AM, Lopez RA, Waseem M, Acute compartment syndrome [Updated 2023 Jan 16]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from:https://www.ncbi.nlm.nih.gov/books/NBK448124/
Figures
Figure 1. Right lower limb swelling and blue discoloration.Figure 2. Computed tomography imaging demonstrating progressive non-opacification of the right infrageniculate arteries. (A) Lower limb computed tomography angiography revealing progressive non-opacification of the right infrageniculate arteries with distal loss of opacification (white arrow). (B) Abdominopelvic computed tomography (cross-sectional view) showing progressive non-opacification of the right infrageniculate arteries (blue arrow).Figure 3. Abdominopelvic computed tomography imaging demonstrating venous thrombosis and associated soft tissue changes. (A) Abdominopelvic computed tomography (sagittal view) showing venous thrombosis extending above the inferior vena cava (IVC) filter (green arrow) into the infrahepatic segment (blue arrow). The IVC filter is visible immediately below the green arrow but not separately labeled. (B) Abdominopelvic computed tomography (cross-sectional view) showing asymmetrical soft tissue enlargement and congestion in the right thigh (yellow arrow). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133