26 July 2025: Articles 
Sacral Neuromodulation for Post-Hysterectomy Hydroureteronephrosis in a Patient with Cervical Cancer: A Case Report
Unusual clinical course, Unusual or unexpected effect of treatment
Fuhao Ji ABEF 1, Lei Xu BDF 1, Jiayi Li ABEF 1*DOI: 10.12659/AJCR.948967
Am J Case Rep 2025; 26:e948967






Abstract
BACKGROUND: Uterine cervical cancer in its early stage is managed with a standard treatment protocol of radical hysterectomy with bilateral pelvic lymphadenectomy. Common complications after the surgery include hydronephrosis, partially leading to renal failure. Currently, there are few reports on upper urinary tract function impairment caused by delayed lower urinary tract dysfunction after radical hysterectomy. Here, we present a case in which sacral neuromodulation (SNM) was successfully used to treat severe hydroureteronephrosis after radical hysterectomy for uterine cervical cancer.
CASE REPORT: A 44-year-old woman was diagnosed with bilateral hydroureteronephrosis and renal insufficiency (serum creatinine at 287 µmol/L) more than 1 year after undergoing radical hysterectomy for uterine cervical cancer. After utilizing an indwelling catheter for 3 months, her renal function showed a progressive improvement and stabilized at around 126 µmol/L. Videourodynamic study (VUDS) indicated decreased bladder compliance, bilateral ureteral reflux, with the reflux graded as IV-V. After confirmation that the upper urinary tract damage was caused by the elevated bladder pressure and not by invasion of the bladder by the primary tumor, SNM was performed to restore lower urinary tract function and to maintain low-pressure urine storage and micturition. Currently, 4 years after the surgery, the creatinine level has progressively declined to 75 µmol/L. Ultrasonography revealed no signs of hydronephrosis. Routine urine tests and post-void residual urine volumes are normal.
CONCLUSIONS: In select patients, sacral neuromodulation can protect the upper urinary tract, probably by improving lower urinary tract function.
Keywords: Hydronephrosis, Hysterectomy, Neurofeedback, Uterine Cervical Neoplasms, Lower urinary tract symptoms, Humans, Female, adult, Electric Stimulation Therapy, Postoperative Complications, Lumbosacral Plexus
Introduction
Uterine cervical cancer in its early stage is managed with a standard treatment protocol of radical hysterectomy with bilateral pelvic lymphadenectomy. The incidence of persistent hydronephrosis in the postoperative period is 15% [1]. In most cases, this hydronephrosis resolves spontaneously, without the need for any clinical intervention [2]. However, in a particular subset of patients, it progresses to severe hydronephrosis, partially leading to renal failure. The underlying mechanisms are multifactorial. During the surgical intervention, the extensive dissection of the peri-vesical and peri-ureteral tissues, combined with thermal injury of the adjacent neuromuscular structures, often is the root cause. These intraoperative factors can cause ureteral stricture or damage the normal function of the lower urinary tract [3]. Currently, there are few reports on upper urinary tract function impairment caused by delayed lower urinary tract dysfunction after radical hysterectomy. Here, we present a case in which sacral neuromodulation (SNM) was successfully used to treat severe hydroureteronephrosis after radical hysterectomy for uterine cervical cancer.
Case Report
A 44-year-old woman was found to have bilateral hydroureteronephrosis accompanied by renal insufficiency more than 1 year after undergoing radical hysterectomy for uterine cervical cancer. At the initial diagnosis, an indwelling urinary catheter was inserted to protect renal function. After 3 months of indwelling catheter use, her renal function improved gradually. The serum creatinine level decreased progressively from 287 μmol/L and stabilized at around 126 μmol/L. Subsequently, a video-urodynamic study (VUDS, Figures 1–3) was performed, which demonstrated decreased bladder compliance (C=6.48 ml/cmH2O). Bilateral ureteral reflux occurred before the bladder was filled to 20 ml, while Pves was 29 cmH2O, and the reflux reached grade IV–V. After shared decision-making (SDM), SNM was performed. During the first year after SNM, an indwelling catheter was utilized to ensure protection of renal function.
Four months after surgery, a follow-up VUDS showed the grade of bladder trabeculation had decreased [4]. The volume at which bilateral ureteral reflux was demonstrated increased from 20 ml to 48 ml, while Pves was 25 cmH2O. At 1-year follow-up, the serum creatinine was 111 μmol/L. VUDS at that time indicated that bladder volume had further increased to 146 ml, while Pves was now 32 cmH2O when right ureteral reflux occurred. No left-sided ureteral reflux occurred, even at the end of the bladder filling phase. Surprisingly, the right-sided ureteral reflux disappeared after the voiding phase. Based on the 1-year follow-up results, the patient’s urinary management was changed from indwelling catheter to clean intermittent self-catheterization (CISC), with a concomitant improvement in quality of life. The patient stopped use of CISC on her own and returned to a completely normal voiding pattern after 3 months and then was lost to follow-up for 1.5 years due to the COVID-19 pandemic. At 2.5 years after the operation, the re-examination of serum creatinine was 87 μmol/L, approaching the normal level, and no hydronephrosis was detected by ultrasound. To date, 4 years after the operation, the creatinine level has progressively declined and is now normal at 75 μmol/L. Routine urine tests and post-void residual urine test results are normal, with no hydronephrosis on ultrasound.
Discussion
We believe that this is the first reported case of applying SNM in a patient with severe hydroureteronephrosis after radical hysterectomy of uterine cervical cancer. After radical hysterectomy, the overall incidence of lower urinary tract dysfunction ranges from 70% to 85% [5]. In the long-term postoperative period, the urodynamic profiles of patients with lower urinary tract dysfunction are predominantly characterized by detrusor underactivity and a low-compliance bladder. The incidence of persistent hydronephrosis following surgery is 15% [1]. To preserve renal function, surgical interventions, including indwelling double-J stents, nephrostomy, ureteroscopic procedures, and surgical reconstruction and repair, are frequently employed for moderate-to-severe upper urinary tract dilation [6]. However, the medical literature on the relationship between lower urinary tract dysfunction and hydronephrosis after uterine cervical cancer surgery remains scant.
In this case, the initial step was to rule out the hypothesis that the invasion of the bladder wall by uterine cervical neoplasms caused a decline in bladder compliance, thereby triggering secondary bladder pressure elevation and subsequent upper urinary tract impairment. At the initial encounter with the patient, an indwelling urinary catheter was inserted. The subsequent partial recovery of the patient’s renal function serves as compelling evidence for a close correlation between upper urinary tract damage and lower urinary tract dysfunction. Furthermore, VUDS disclosed bilateral ureteral reflux before bladder filling to 20 ml, which provides strong evidence for the close connection between upper and lower urinary tract dysfunction. Consequently, for this patient, the critical strategy for safeguarding renal function was restoring lower urinary tract function to maintain low-pressure urine storage and micturition.
Oral anticholinergic medications can be administered to decrease the intravesical pressure during the filling phase [7,8]. Combined with CISC, with which the bladder can be emptied under low-pressure conditions, this can safeguard the upper urinary tract. Additionally, CISC can shorten the cumulative duration of catheterization and facilitate recovery of bladder function [9]. Zullo et al reported the incidence of urinary retention following radical hysterectomy for uterine cervical cancer ranges from 8% to 80%, which can achieve complete restoration within 9–12 months after surgery [10]. Clean intermittent catheterization is the preferred management for neuro-urological patients who cannot effectively empty their bladders, and the optimal frequency of catheterization carried out daily is approximately 5 times [11]. However, in the present case, ureteral reflux occurred when the bladder was filled to 20 ml, meaning that the patient theoretically needed to perform CISC every time the bladder filled to 20 ml, which is not operationally achievable. This practical challenge renders the implementation of such a treatment regimen unfeasible [12].
Entero-cystoplasty can enlarge the bladder, enabling low-pressure urine storage. After the operation, it can be combined with CISC to assist in low-pressure bladder emptying. However, entero-cystoplasty has substantial surgical risks, and the potential occurrence of surgical complications can precipitate alterations in intestinal and urinary system functions. Furthermore, the modifications in the anatomical structure and the obligatory postoperative CISC invariably decrease the quality of life. The overall 5-year relative survival rate of patients with uterine cervical cancer is 67%, accompanied by a risk of tumor recurrence. Subsequent radiotherapy and chemotherapy may be necessary, potentially exerting unforeseen effects on the augmented bladder [13]. Thus, for this patient, determining whether entero-cystoplasty confers more benefits than drawbacks or vice versa poses a challenging decision-making scenario.
SNM, via low-intensity electrical impulses, modulates the neural innervation of the pelvic floor and lower urinary tract, aiming to partially restore the patient’s lower urinary tract dysfunction. This intervention is indicated for frequency, urgency, urge urinary incontinence, and non-obstructive urinary retention, which means it has bidirectional regulation for filling and voiding phases of micturition. EAU guidelines recommend that SNM can be considered as an active transitional treatment or trial before more invasive surgeries such as bladder augmentation or urinary diversion [11]. After shared decision-making (SDM), all critically important and relevant information was meticulously communicated to the patient and her family to ensure they could make well-informed decisions, and then the patient explicitly expressed willingness to undergo SNM prior to more invasive surgeries.
After SNM surgery, management was guided by the results of the follow-up-VUDS. The lower urinary tract function was closely monitored to ensure protection of renal function. The patient had an indwelling catheter for 1 year, and then CISC for 3 months, then returned to spontaneous urination. Results of 4-year follow-up verified that the intervention achieved the anticipated outcomes. Currently, the patient’s clinical parameters have normalized, with no evidence of hydronephrosis, and she can void spontaneously and was able to resume normal activities.
Prior to the operation, we consulted the patient’s attending gynecologist and ascertained that alternative tumor surveillance methods could substitute for postoperative MRI following SNM. To date, there has been no recurrence of the tumor.
It is impossible to conclude that all patients with similar presentations will uniformly benefit from the same procedure, as the outcome is highly individualized and contingent on multiple factors. Each patient’s condition and response to treatment vary significantly, underscoring the need for further exploration and research in this field. Additionally, personalized management plans, along with close follow-up by specialized physicians, are essential to optimize patient care and outcomes. Such an approach will help in better understanding the efficacy and applicability of the procedure across different patient populations, thereby facilitating the development of more targeted and effective treatment strategies.
Conclusions
To the best of our knowledge, this is the first report demonstrating that sacral neuromodulation therapy, in combination with suitable catheterization approaches, including indwelling urinary catheter and clean intermittent self-catheterization, can protect the upper urinary tract, probably by improving lower urinary tract function, and urinary catheter removal can be considered when SNM takes effect.
Figures
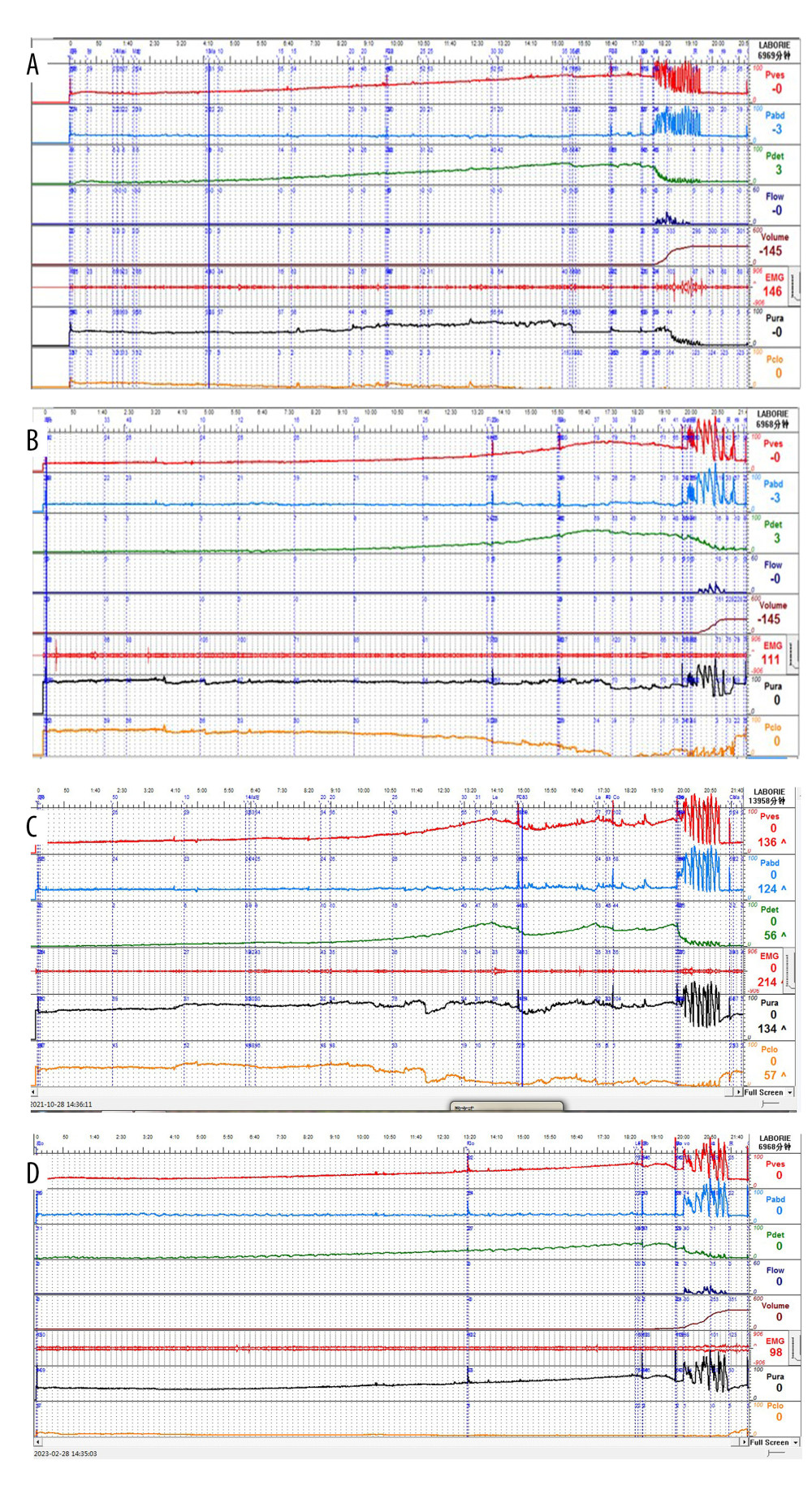 Figure 1. VUDS curve: Pre-operation (C=6.48 ml/cmH2O) (A), 4 months after operation (B), 1 year after operation (C), and 2.5 years after operation (C=8.04 ml/cmH2O) (D)
Figure 1. VUDS curve: Pre-operation (C=6.48 ml/cmH2O) (A), 4 months after operation (B), 1 year after operation (C), and 2.5 years after operation (C=8.04 ml/cmH2O) (D) 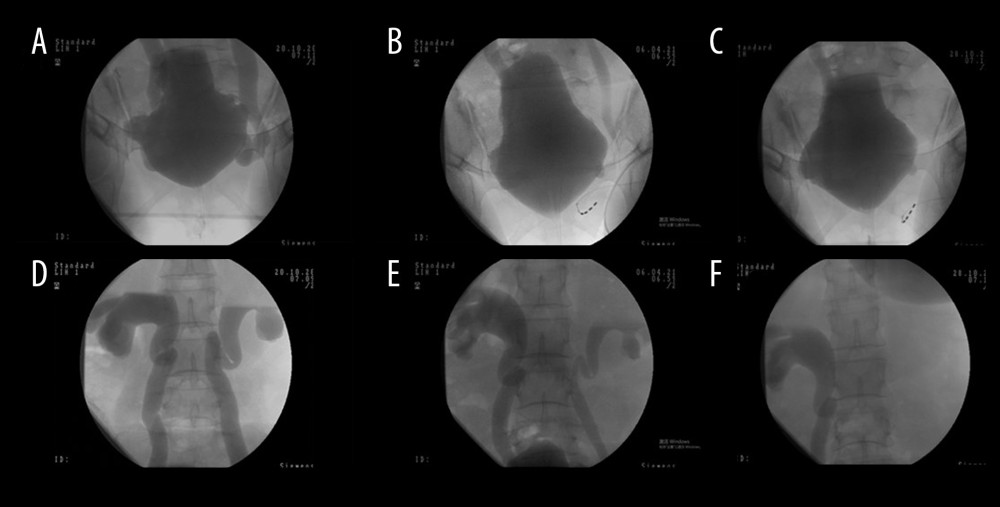 Figure 2. Bladder morphology and ureteral reflux under X-ray at the end of the filling phase of VUDS: Pre-operation (A, D), 4 months after operation (B, E), and 1 year after operation (C, F).
Figure 2. Bladder morphology and ureteral reflux under X-ray at the end of the filling phase of VUDS: Pre-operation (A, D), 4 months after operation (B, E), and 1 year after operation (C, F). 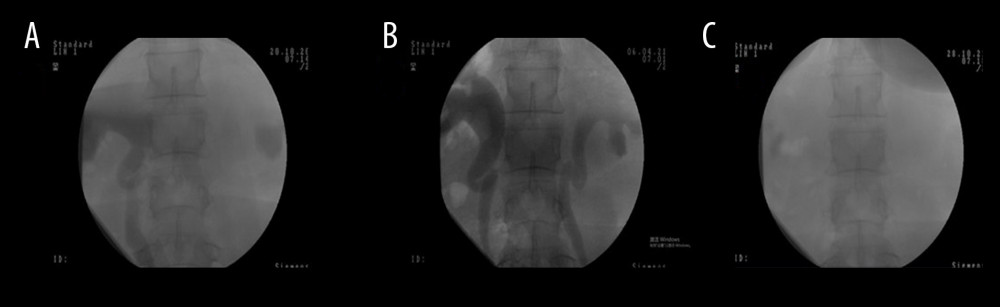 Figure 3. X-ray of the upper urinary tract at the end of voiding phase of VUDS: Pre-operation (A), 4 months after operation (B), and 1 year after operation (C).
Figure 3. X-ray of the upper urinary tract at the end of voiding phase of VUDS: Pre-operation (A), 4 months after operation (B), and 1 year after operation (C). References
1. Patel K, Foster NR, Kumar A, Hydronephrosis in patients with cervical cancer: An assessment of morbidity and survival: Support Care Cancer, 2015; 23(5); 1303-9
2. Paick SH, Oh SJ, Song YS, The natural history of hydronephrosis after radical hysterectomy with no intraoperatively recognisable injury to the ureter: A prospective study: BJU Int, 2003; 92(7); 748-50
3. Suprasert P, Euathrongchit J, Suriyachai P, Hydronephrosis after radical hysterectomy: A prospective study: Asian Pac J Cancer Prev, 2009; 10(3); 375-78
4. Cho SY, Bae J, Yoo C, Establishment of a grading system for bladder trabeculation: Urology, 2013; 81(3); 503-7
5. Wit EM, Horenblas S, Urological complications after treatment of cervical cancer: Nat Rev Urol, 2014; 11(2); 110-17
6. Nobrega L, Zanon JR, Andrade C, Prognostic role of hydronephrosis in the treatment of patients with locally advanced cervical cancer: A retrospective cohort: Int J Gynecol Cancer, 2022; 32(9); 1123-28
7. Aue-Aungkul A, Kietpeerakool C, Rattanakanokchai S, Postoperative interventions for preventing bladder dysfunction after radical hysterectomy in women with early-stage cervical cancer: Cochrane Database Syst Rev, 2021; 1(1); CD012863
8. Sirisreetreerux P, Wattanayingcharoenchai R, Rattanasiri S, Medical and non-medical interventions for post-operative urinary retention prevention: Network meta-analysis and risk-benefit analysis: Ther Adv Urol, 2021; 13; 17562872211022296
9. Wand J, Feng M, Liao T, Effects of clean intermittent catheterization and transurethral indwelling catheterization on the management of urinary retention after gynecological surgery: A systematic review and meta-analysis: Transl Androl Urol, 2023; 12(5); 744-60
10. Zullo MA, Manci N, Angioli R, Vesical dysfunctions after radical hysterectomy for cervical cancer: A critical review: Crit Rev Oncol Hematol, 2003; 48(3); 287-93
11. EAU Guidelines
12. Seth JH, Haslam C, Panicker JN, Ensuring patient adherence to clean intermittent self-catheterization: Patient Prefer Adherence, 2014; 8; 191-98
13. Li J, LuU G, Luo J, Cervical cancer prognosis and related risk factors for patients with cervical cancer: A long-term retrospective cohort study: Sci Rep, 2022; 12(1); 13994
Figures
Figure 1. VUDS curve: Pre-operation (C=6.48 ml/cmH2O) (A), 4 months after operation (B), 1 year after operation (C), and 2.5 years after operation (C=8.04 ml/cmH2O) (D)Figure 2. Bladder morphology and ureteral reflux under X-ray at the end of the filling phase of VUDS: Pre-operation (A, D), 4 months after operation (B, E), and 1 year after operation (C, F).Figure 3. X-ray of the upper urinary tract at the end of voiding phase of VUDS: Pre-operation (A), 4 months after operation (B), and 1 year after operation (C). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133