09 December 2025: Articles 
A Rare Case of Emphysematous Pyelonephritis Following Retrograde Intrarenal Surgery in an Elderly Man
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Weiyong ZhongDOI: 10.12659/AJCR.949018
Am J Case Rep 2025; 26:e949018






Abstract
BACKGROUND: Emphysematous pyelonephritis (EPN) is a severe, rare urinary tract infection (UTI) primarily affecting patients with diabetes or compromised immune function. Characterized by nonspecific manifestations including fever, flank pain, and pyuria, it frequently overlaps with other renal or abdominal conditions, leading to diagnostic delays and increased mortality risk. Notably, EPN following retrograde intrarenal surgery (RIRS) – a minimally invasive technique for renal and ureteral stone management – is extremely rare, with no prior documented cases in the literature.
CASE REPORT: A 74-year-old Chinese man was admitted on May 15, 2024 due to a >3-cm right ureteropelvic junction stone, multiple right renal stones, and concurrent right renal hydronephrosis. Preoperative urine culture identified Klebsiella aerogenes and Citrobacter koseri, prompting 9 days of perioperative levofloxacin (500 mg/day), which cleared the infection. Despite guideline recommendations for percutaneous nephrolithotomy, he opted for RIRS, undergoing first-stage surgery with double-J catheter placement on May 24 and discharging uneventfully on May 27. On postoperative day 10 (June 3), he developed a 39°C fever and persistent abdominal pain. CT confirmed Grade 1 EPN, ureteral steinstrasse, and persistent hydronephrosis. Urgent percutaneous nephrostomy, catheter replacement, and 11-day ertapenem therapy (1g/day) controlled the infection, and a second RIRS on June 12 cleared the stones, with no complications in 3-month follow-up.
CONCLUSIONS: Post-RIRS fever/abdominal pain requires urgent imaging to rule out steinstrasse-induced EPN. Early drainage, targeted antibiotics, and staged RIRS are critical for elderly patients with high stone burden, filling the literature gap on this complication.
Keywords: Ureteroscopy, Pyelonephritis, Enterobacter aerogenes, Urinary Calculi, Urinary Tract Infections, Humans, Male, Aged, emphysema, Postoperative Complications, Kidney Calculi, Anti-Bacterial Agents, Enterobacteriaceae Infections, emphysematous pyelonephritis
Introduction
Retrograde intrarenal surgery (RIRS) is a minimally invasive, widely-used technique for managing renal and ureteral stones [1–3]. Despite its advantages, including rapid recovery and reduced morbidity, postoperative complications such as ureteral injury, infection, and stricture formation remain concerns [3,4]. Among these, emphysematous pyelonephritis (EPN) – a rare, life-threatening bacterial infection characterized by gas accumulation in the renal parenchyma and peri-renal tissues – is an exceptionally uncommon complication [5]. EPN predominantly affects patients with diabetes mellitus or immunocompromised states, with pathogenesis involving hyperglycemia-induced tissue hypoxia, urinary obstruction, and bacterial virulence factors [6,7]. Clinical presentation is often nonspecific (fever, flank pain, pyuria), necessitating imaging (eg, computed tomography [CT]) for definitive diagnosis, which typically reveals renal parenchymal gas [6,8]. While EPN has been reported after ureteroscopy, its occurrence after RIRS is exceedingly rare, with no prior documented cases in the literature (Table 1). Risk factors include intraoperative mucosal trauma, postoperative urinary stasis, and patient comorbidities. Early recognition and intervention are critical to mitigate mortality. Management strategies include prompt drainage (eg, percutaneous nephrostomy), broad-spectrum antibiotics, and definitive stone clearance.
Here, we report a case of EPN complicating RIRS in a 74-year-old man with ureteral steinstrasse and multiple renal stones. He was successfully treated with nephrostomy, antibiotic therapy (ertapenem), and staged RIRS, highlighting the importance of vigilance for obstructive complications in high-risk patients.
Case Report
PATIENT INFORMATION:
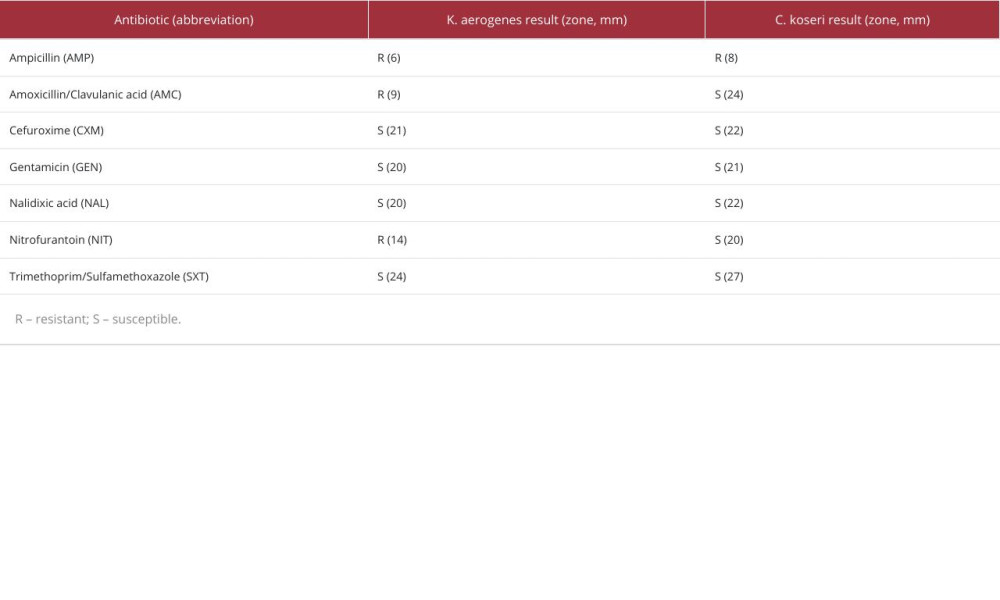
This case involves a 74-year-old Chinese man who was admitted on May 15, 2024 due to a huge right ureteropelvic junction stone, multiple right renal stones, and hydronephrosis of the right kidney (Figure 1A–1C). Urine culture showed the presence of Klebsiella aerogenes and Citrobacter koseri. Antimicrobial susceptibility was determined by Kirby-Bauer disk diffusion in accordance with CLSI M100 standards. Results are summarized in Table 2. Given the high risk of urinary tract infection (UTI), levofloxacin was administered at a dose of 500 mg per day during the perioperative period, with the treatment lasting 9 days (May 15 to May 23). The urine culture was negative on May 23. According to urinary calculi management guidelines, percutaneous nephrolithotomy (PCNL) is recommended. After providing the patient with detailed information about the condition, he requested RIRS. Considering that the maximum diameter of the stone was greater than 3 cm, we planned to perform staged ureteroscopic lithotripsy, and on May 24 a first-stage right RIRS+right double-J catheter placement was performed (Figure 1D). The postoperative recovery was smooth, with no significant bleeding, infection, or other complications. The patient was discharged on May 27.
On June 3, 2024, he developed a fever with a maximum temperature of 39°C and lower abdominal distension and pain. After being admitted to the hospital, a CT scan (Figure 2A) was performed, which showed gas accumulation in the right renal pelvis, accompanied by a right ureteral stone and hydronephrosis of the right kidney. Laboratory data indicate a significant elevation in the patient’s inflammatory markers in blood tests. (WBC: 15.19×109/L, CRP: 118.63 mg/L, PCT: 0.27 ng/ml, IL-6: 50.9 pg/ml). Blood culture (aerobic/anaerobic) was negative, and a urine culture (midstream clean-catch specimen) showed no pathogenic bacteria growth. We considered a diagnosis of EPN (Grade 1), right ureteral steinstrasse, and multiple right renal stones. Immediate right percutaneous nephrostomy and right double-J catheter replacement were performed, and ertapenem was administered at a dose of 1 g per day for 11 days (June 3 to June 13). Postoperatively, body temperature gradually returned to normal, and the infection was effectively controlled. On June 12, 2024, he underwent a right RIRS and right double-J catheter replacement. A postoperative follow-up CT scan (Figure 2B) showed reduced dilation of the right renal pelvis and absorption of gas in the right renal pelvis, and the multiple stones in the right kidney and the right ureter stone street had disappeared.
FOLLOW-UP SITUATION:
Postoperative outpatient follow-up was conducted over a period of 3 months (June 15 to September 15, 2024). During this period, the patient reported no significant discomfort and experienced no episodes of fever. Serial imaging examinations (ultrasound at 1 month and non-contrast CT at 3 month) showed no residual stones. No long-term complications such as ureteral stricture or recurrent infection were observed.
Discussion
Emphysematous pyelonephritis (EPN) is a severe, gas-forming UTI characterized by microbial production of gas within the renal parenchyma and collecting system [9,10]. EPN is classified into 4 grades by CT findings (Grade 1: gas confined to the collecting system; Grade 2: gas in renal parenchyma without perirenal extension; Grade 3A: gas/abscess extending to perirenal space; Grade 3B: gas/abscess involving perinephric space; and Grade 4: bilateral EPN or EPN in a solitary kidney) [11]. EPN is rare in routine urinary infections but is more prevalent in immunocompromised patients and post-urinary-surgical settings, including kidney transplantation [12–15]. Notably, its occurrence after retrograde intrarenal surgery (RIRS) is exceedingly rare, with no prior reported cases, making this a clinically significant case report.
EPN development hinges on 3 key factors: gas-producing bacteria (eg,
Notably, on the day of EPN diagnosis (postoperative day 10), the patient’s blood culture (aerobic/anaerobic, 48-h incubation) and urine culture (midstream clean-catch, blood/MacConkey agar) both showed no pathogenic growth. This negative result, despite radiological EPN confirmation, may stem from 3 factors: 1) Residual levofloxacin from preoperative 9-day therapy inhibited pathogen growth in culture; 2) Ureteral steinstrasse trapped infected urine in the upper urinary tract, leading to insufficient bacteria in the lower-tract urine specimen; and 3) Specimen collection at 6 h after fever onset (early EPN stage) preceded bacterial proliferation peaks. This emphasizes that negative urine culture should not rule out EPN in post-RIRS patients – diagnosis must rely on clinical manifestations, inflammatory markers, and radiology.
Ureteral steinstrasse – a post-lithotripsy obstruction caused by fragmented stone accumulation in the ureter [16–18] – was a pivotal contributor in this case. Risk factors for steinstrasse include large stone burden (>2 cm), high stone density (CT value), incomplete fragmentation, excessive early patient activity, and suboptimal intraoperative stone clearance [16–18]. Here, the 3-cm UPJ stone, excessive fragmentation during flexible RIRS (resulting in retained large fragments), and insufficient intraoperative extraction likely precipitated steinstrasse. This highlights the imperative for maximal intraoperative stone removal, particularly for large calculi in high-risk patients.
The mortality of EPN ranges from 11% to 90%, with higher rates in type I/classic EPN or bilateral involvement [19]. Key predictors include thrombocytopenia, uncontrolled diabetes, obstructive uropathy, DIC, and extensive gas spread [20,21]. A recent 0–7 risk score system stratifies mortality: scores ≤3 predict 83% [21]. Treatment emphasizes rapid risk assessment: non-obstructed EPN is managed with antibiotics (eg, carbapenems/3rd–/4th-gen cephalosporins) and percutaneous drainage (70–90% success) [22]; obstruction requires urgent decompression (ureteral stenting/nephrostomy within 48 h), as delays >48 h increase mortality by 44% to 69% [23,24]. Nephrectomy is reserved for failed conservative management or grade 3 EPN with sepsis [25].
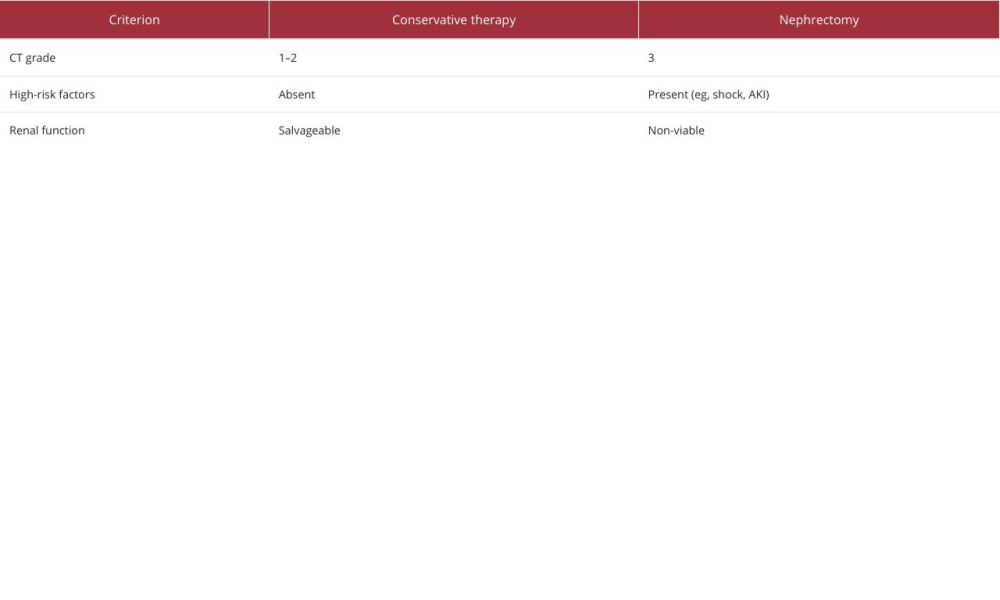
While intraoperative stone clearance prevents EPN, established EPN necessitates risk-adapted decisions. In this case, conservative therapy (antibiotics + percutaneous drainage) was prioritized over nephrectomy based on 3 evidence-backed criteria: 1) Low-grade EPN (CT Grade 1) without perinephric extension, correlating with 15% to 20% mortality under conservative therapy versus >40% in Grade 3 [6,26]; 2) Absence of high-risk predictors: Thrombocytopenia (<100,000/mm3), AKI (creatinine >3.0 mg/dL), or shock [26,27]; and 3) Salvageable solitary kidney (contralateral atrophy), where nephrectomy mandates lifelong dialysis [28]. Strict nephrectomy triggers are: 1) Persistent fever/leukocytosis >72 h [27]; 2) Perinephric gas on repeat imaging [6]; and 3) Hemodynamic instability [26,28]. Table 3 contrasts key decision indicators. This aligns with modern paradigms: organ preservation is feasible for low-grade EPN without risk factors, while emergency nephrectomy remains the standard for advanced disease.
EPN’s nonspecific symptoms (fever, flank pain, pyuria) often mimic uncomplicated pyelonephritis or acute abdominal pathology (eg, appendicitis, diverticulitis), leading to diagnostic delays. In this patient, rapid progression from fever to gas accumulation on CT (within 10 days after RIRS) underscores the necessity for early imaging in symptomatic post-RIRS patients, even without overt obstruction signs. This risk-adapted approach emphasizes that delayed diagnosis significantly increases mortality, mandating low-threshold imaging in atypical cases.
Conclusions
The cornerstones of EPN treatment are prompt drainage (percutaneous nephrostomy or ureteral stenting), targeted antibiotics, and definitive stone clearance. In this case, immediate nephrostomy, DJ stent replacement, and ertapenem therapy effectively controlled infection, followed by staged RIRS for residual stones, leading to full recovery. This case report shows that post-RIRS fever and abdominal pain should prompt consideration of urgent imaging to exclude obstructive complications that can precipitate EPN, and high stone burden and incomplete intraoperative clearance increase steinstrasse risk, necessitating aggressive fragmentation and extraction.
Further studies are needed to define surveillance protocols for high-risk post-RIRS patients, but this case report provides a valuable framework for early recognition and management of this rare, life-threatening complication.
Figures
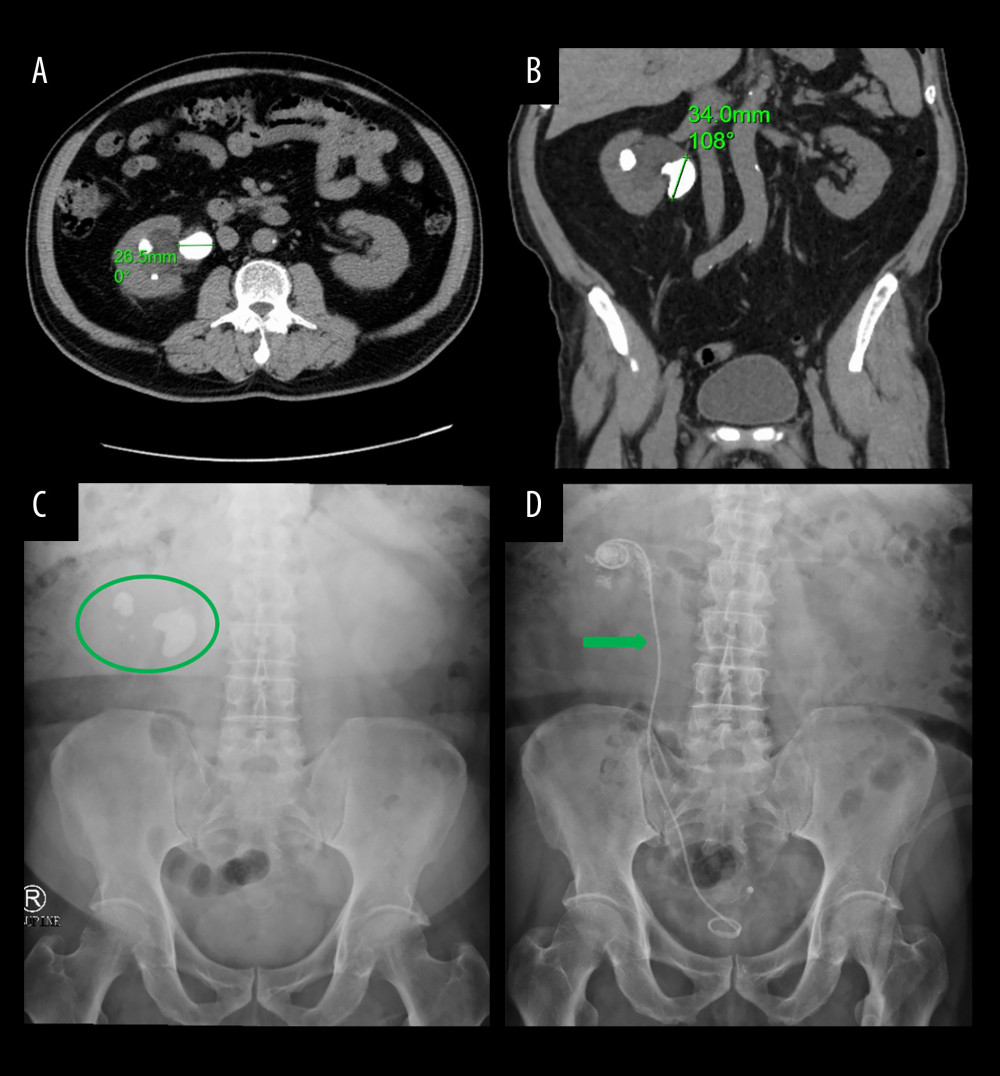 Figure 1. Preoperative imaging findings of right renal and ureteral stones. CT scans: (A) Axial view showing the stone (longest axis marked with green numbers). (B) Coronal view of the right kidney. KUB X-ray: (C) Multiple right renal stones (green circles). (D) Ureteral stent placement (green arrow).
Figure 1. Preoperative imaging findings of right renal and ureteral stones. CT scans: (A) Axial view showing the stone (longest axis marked with green numbers). (B) Coronal view of the right kidney. KUB X-ray: (C) Multiple right renal stones (green circles). (D) Ureteral stent placement (green arrow). 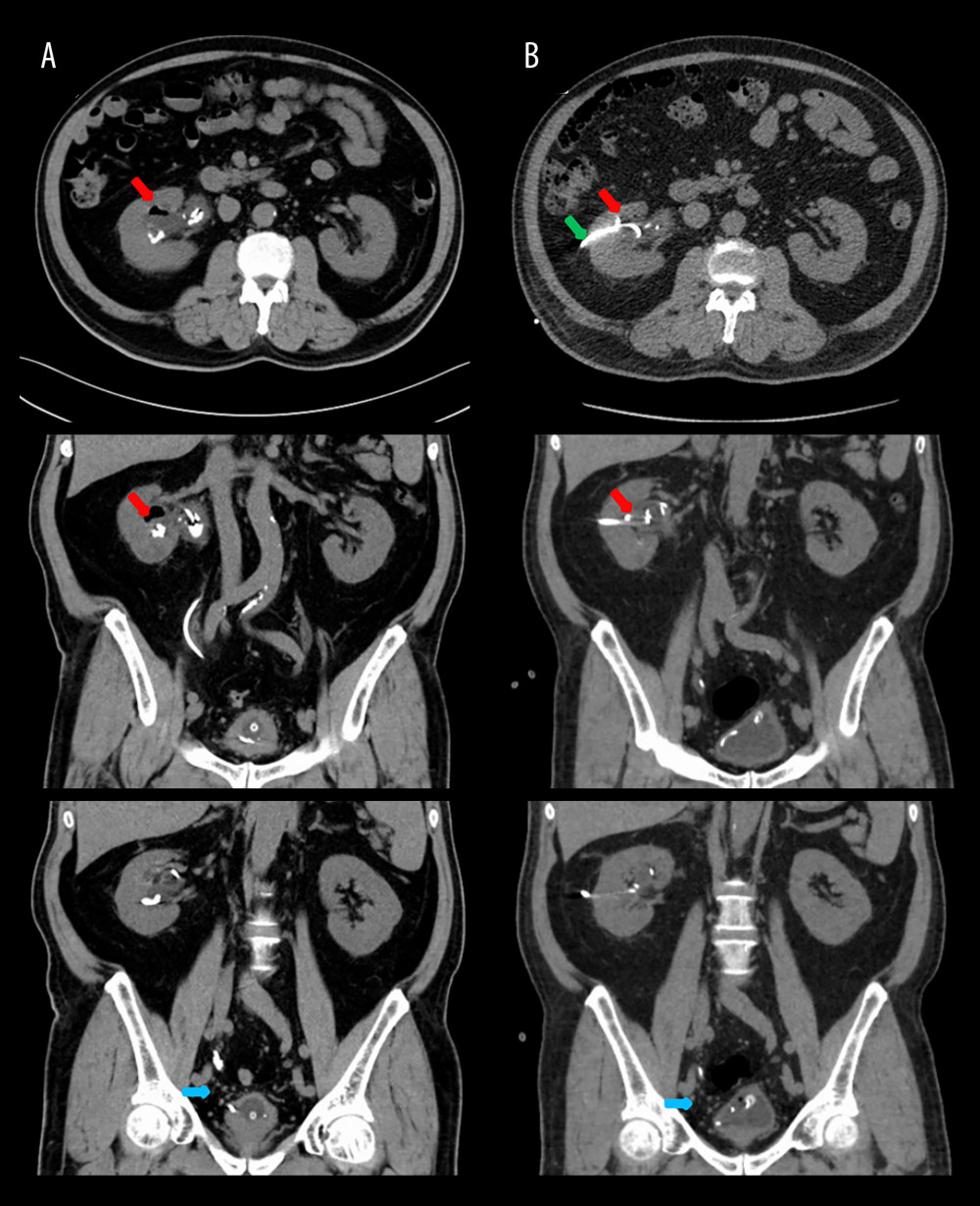 Figure 2. Imaging changes before and after nephrostomy with secondary RIRS. (A) Admission CT scans: (Top) Axial view and (Middle) coronal view demonstrating right pneumopyelia (red arrows), (Bottom) coronal view showing mid-right ureteral steinstrasse. (B) Postoperative CT scans: (Top) Axial view and (Middle) coronal view revealing resolution of pneumopyelia (red arrows) and nephrostomy tube placement (green arrow), (Bottom) coronal view confirming complete clearance of ureteral steinstrasse.
Figure 2. Imaging changes before and after nephrostomy with secondary RIRS. (A) Admission CT scans: (Top) Axial view and (Middle) coronal view demonstrating right pneumopyelia (red arrows), (Bottom) coronal view showing mid-right ureteral steinstrasse. (B) Postoperative CT scans: (Top) Axial view and (Middle) coronal view revealing resolution of pneumopyelia (red arrows) and nephrostomy tube placement (green arrow), (Bottom) coronal view confirming complete clearance of ureteral steinstrasse. 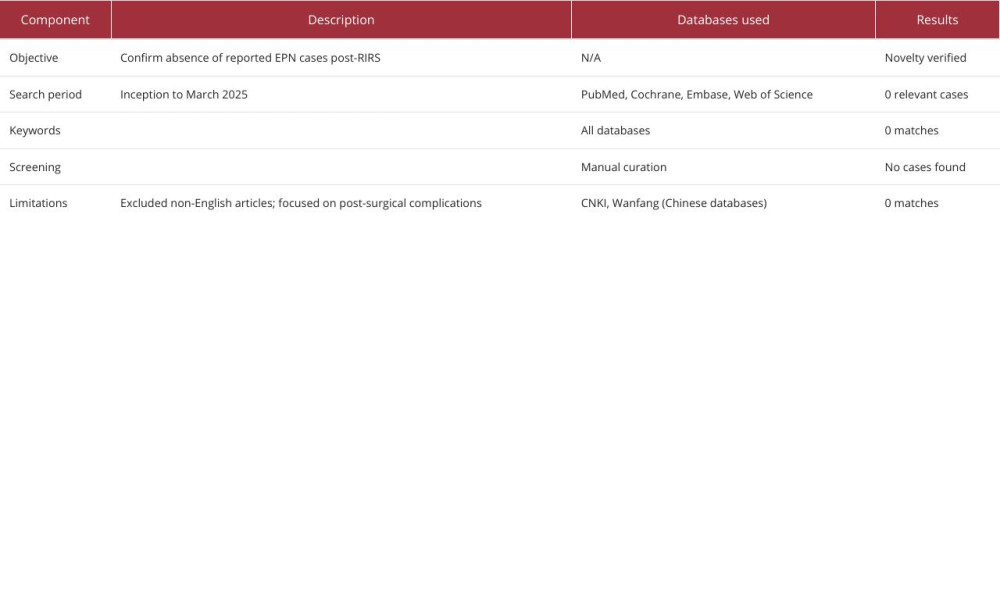
References
1. Setthawong V, Srisubat A, Potisat S, Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones: Cochrane Database Syst Rev, 2023; 8(8); CD007044
2. Soderberg L, Ergun O, Ding M, Percutaneous nephrolithotomy versus retrograde intrarenal surgery for treatment of renal stones in adults: Cochrane Database Syst Rev, 2023; 11(11); CD013445
3. He M, Dong Y, Cai W, Recent advances in the treatment of renal stones using flexible ureteroscopys: Int J Ssurg, 2024; 110(7); 4320-28
4. Jiang CY, Shao Y, Xia SJFocus on complications of flexible ureteroscopic lithotripsy: Zhonghua Yi Xue Za Zhi, 2019; 99(6); 404-6 [in Chinese]
5. Ubee SS, McGlynn L, Fordham M, Emphysematous pyelonephritis: BJU Int, 2011; 107(9); 1474-78
6. Wu SY, Yang SS, Chang SJ, Hsu CK, Emphysematous pyelonephritis: Classification, management, and prognosis: Tzu Chi Med J, 2022; 34(3); 297-302
7. Rafiq N, Nabi T, Rasool S, Sheikh RY, A prospective study of emphysematous pyelonephritis in patients with type 2 diabetes: Indian J Nephrol, 2021; 31(6); 536-43
8. Pontin AR, Barnes RD, Current management of emphysematous pyelonephritis: Na Rev Urol, 2009; 6(5); 272-79
9. Schneeberger C, Holleman F, Geerlings SE, Febrile urinary tract infections: Pyelonephritis and urosepsis: Curr Opin Infect Dis, 2016; 29(1); 80-85
10. Sherchan R, Hamill R: Emphysematous pyelonephritis. StatPearls Treasure Island (FL) ineligible companies. Disclosure: Richard Hamill declares no relevant financial relationships with ineligible companies, 2025, StatPearls Publishing. Copyright © 2025, StatPearls Publishing LLC
11. Huang JJ, Tseng CC, Emphysematous pyelonephritis: Clinicoradiological classification, management, prognosis, and pathogenesis: Arch Intern Med, 2000; 160(6); 797-805
12. Tangirala N, Singer J, Snelling P, Emphysematous pyelonpehritis in a dual kidney transplant recipient: Nephrology (Carlton), 2018; 23(11); 1064-65
13. Chouaib A, Sebe P, Haab F, Tligui MEmphysematous pyelonephritis in a kidney allograft: indication for a secondary nephrectomy: Med Mal Infect, 2011; 41(8); 443-45 [in French]
14. Bansal RK, Lambe S, Kapoor A, Emphysematous pyelonephritis in failed renal allograft: Case report and review of literature: Urol Ann, 2016; 8(1); 111-13
15. Schmidt S, Foert E, Zidek W, Emphysematous pyelonephritis in a kidney allograft: Am J Kidney Dis, 2009; 53(5); 895-97
16. Sullere A, Sureka B, Khera PS, ‘Stone street’ ureter: Abdom Radiol (NY), 2018; 43(8); 2204-5
17. Birowo P, Rasyid N, Atmoko W, Sutojo B, Case Report: An occurrence of steinstrasse in retrograde intra renal surgery (RIRS) for large staghorn kidney stone: A difficult experience in managing surgical outcomes: F1000Res, 2020; 9; 184
18. Ibrahim RM, Sayed O, Lotfy AM, Extracorporeal shock wave lithotripsy versus laser lithotripsy in the treatment of post-SWL steinstrasse: A randomized comparative study: World J Urol, 2024; 42(1); 345
19. Misgar RA, Mubarik I, Wani AI, Emphysematous pyelonephritis: A 10-year experience with 26 cases: Indian J Endocrinol Metab, 2016; 20(4); 475-80
20. Aggarwal D, Mandal S, Parmar K, Predictors of mortality and nephrectomy in emphysematous pyelonephritis: A tertiary care centre study: Ann R Coll Surg Engl, 2023; 105(4); 323-30
21. Trujillo-Santamaría H, Robles-Torres JI, Teoh JY, A novel mortality risk score for emphysematous pyelonephritis: A multicenter study of the Global Research in the Emphysematous Pyelonephritis group: Curr Urol, 2024; 18(1); 55-60
22. Chen MT, Huang CN, Chou YH, Percutaneous drainage in the treatment of emphysematous pyelonephritis: 10-year experience: J Urol, 1997; 157(5); 1569-73
23. Zul Khairul Azwadi I, Norhayati MN, Abdullah MS, Percutaneous nephrostomy versus retrograde ureteral stenting for acute upper obstructive uropathy: A systematic review and meta-analysis: Sci Rep, 2021; 11(1); 6613
24. Lu YC, Chiang BJ, Pong YH, Emphysematous pyelonephritis: Clinical characteristics and prognostic factors: Int J Urol, 2014; 21(3); 277-82
25. Desai R, Batura D, A systematic review and meta-analysis of risk factors and treatment choices in emphysematous pyelonephritis: Int Urol Nephrol, 2022; 54(4); 717-36
26. Raina S, Diabetes, fever and flank pain: Is it emphysematous pyelonephritis?: J Family Med Prim Care, 2012; 1(2); 157-59
27. Sengupta S, Basu S, Outcome of conservative and minimally invasive management in emphysematous pyelonephritis: Urol Ann, 2021; 13(3); 277-81
28. Kutwin P, Konecki T, Jabłonowski Z, Emphysematous pyelonephritis in a diabetic patient with obstructed kidney: Cent European J Urol, 2014; 67(2); 196-98
Figures
Figure 1. Preoperative imaging findings of right renal and ureteral stones. CT scans: (A) Axial view showing the stone (longest axis marked with green numbers). (B) Coronal view of the right kidney. KUB X-ray: (C) Multiple right renal stones (green circles). (D) Ureteral stent placement (green arrow).Figure 2. Imaging changes before and after nephrostomy with secondary RIRS. (A) Admission CT scans: (Top) Axial view and (Middle) coronal view demonstrating right pneumopyelia (red arrows), (Bottom) coronal view showing mid-right ureteral steinstrasse. (B) Postoperative CT scans: (Top) Axial view and (Middle) coronal view revealing resolution of pneumopyelia (red arrows) and nephrostomy tube placement (green arrow), (Bottom) coronal view confirming complete clearance of ureteral steinstrasse. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133