15 December 2025: Articles 
Primary Pulmonary Osteosarcoma Presenting as a 1.7-cm Subpleural Nodule in a 61-Year-Old Man: A Case Report
Unusual clinical course, Challenging differential diagnosis, Rare disease
Xin Yang ABCDEF 1, Wen Guang Zhao BCF 1, Chao Gao ABC 1, Sheng Lin CDF 1,2*DOI: 10.12659/AJCR.949034
Am J Case Rep 2025; 26:e949034






Abstract
BACKGROUND: Primary pulmonary osteosarcoma (PPOS) is rare and can mimic metastases or benign pulmonary nodules. We present a 1.7-cm PPOS and outline an imaging-pathology diagnostic workup.
CASE REPORT: A 61-year-old man with prior hepatocellular carcinoma (HCC) developed a right upper lobe subpleural nodule enlarging from 0.7 to 1.7 cm over 5 months. Positron emission tomography/computed tomography showed moderate uptake (SUVmax=5.2). Whole-body bone scintigraphy showed no skeletal lesions. Uniportal video-assisted thoracoscopic wedge resection with lymph node sampling was performed, with negative margins. Histologic examination revealed a spindle-cell sarcoma producing lace-like malignant osteoid with a focal chondroid matrix. Immunohistochemistry showed diffuse nuclear special AT-rich sequence-binding protein 2 (SATB2) positivity, with a Ki-67 index of approximately 30%, while epithelial, vascular, and solitary fibrous tumor markers were negative. Although HCC-specific immunohistochemistry was not performed, normal alpha-fetoprotein levels, the absence of hepatic recurrence on imaging, and the presence of malignant osteoid formation supported the exclusion of metastatic HCC. A final diagnosis of PPOS was made. The patient received adjuvant liposomal doxorubicin plus cisplatin and, to date, remained disease-free 9 months after surgery.
CONCLUSIONS: PPOS can present as a lesion smaller than 2 cm. An integrated imaging-pathology workup and early resection can yield favorable short-term outcomes.
Keywords: Osteosarcoma, Pathological Conditions, Signs and Symptoms, Immunohistochemistry, surgical oncology, lung neoplasms, Humans, Male, Middle Aged, Carcinoma, Hepatocellular, Liver Neoplasms, Thoracic Surgery, Video-Assisted, Radionuclide Imaging, Positron Emission Tomography Computed Tomography, Diagnosis, Differential, Neoplasms, Second Primary, Chemotherapy, Adjuvant, Lung
Introduction
Primary pulmonary osteosarcoma (PPOS) is an exceedingly rare malignant neoplasm, constituting approximately 0.01% of all primary pulmonary tumors [1,2]. The rarity is compounded by diagnostic complexities, as PPOS often mimics metastatic lesions or benign pulmonary nodules, leading to significant clinical challenges [1]. Historically, in patients with PPOS, the size of tumors at the first visit mostly exceeded 5 cm, and tumors larger than 5 cm were usually associated with a poor prognosis [2,3].
Clinically, PPOS presents with nonspecific symptoms, such as chest pain, cough, and hemoptysis. These features overlap with common pulmonary diseases, complicating diagnosis [1,2]. Differential diagnosis is particularly arduous, requiring exclusion of metastatic osteosarcoma, primary lung carcinomas, and benign osseous lesions [3,4]. Key diagnostic steps include whole-body imaging, such as with positron emission tomography/computed tomography (PET/CT) and bone scintigraphy, to rule out extrapulmonary primary sites and immunohistochemistry (IHC) to confirm osteoblastic differentiation, such as special AT-rich sequence-binding protein 2 (SATB2) positivity [2,5,6]. The coexistence of comorbid malignancies, such as hepatocellular carcinoma (HCC) in this case, further complicates the interpretation of imaging findings, necessitating integrated multimodal approaches. These challenges highlight the critical role of multidisciplinary collaboration-combining radiological, pathological, and clinical expertise-to avoid misclassification and facilitate timely intervention. Complete resection is the mainstay of management, while evidence for adjuvant chemotherapy remains limited due to the rarity of PPOS [1,3]. This report describes the case of a 61-year-old man with a 1.7-cm PPOS in the right upper lobe, highlighting the diagnostic challenges and management approach.
Case Report
A 61-year-old man with a history of poorly differentiated HCC, treated with left lateral lobectomy and transarterial chemoembolization in February 2020, was under regular surveillance. In August 2024, a computed tomography (CT) scan incidentally detected a 0.7-cm, well-circumscribed, smooth-edged subpleural nodule in the posterior segment of the right upper lobe (Figure 1A). The lesion was considered radiologically benign, and follow-up was recommended.
In January 2025, a follow-up CT scan showed that the nodule had enlarged to 1.7 cm (Figure 1B). Subsequently, PET/CT was performed, revealing increased metabolic activity within the nodule, with a maximum standardized uptake value (SUVmax) of 5.2 (Figure 1C). Whole-body bone scintigraphy showed no evidence of skeletal uptake or other extrapulmonary lesions (Figure 1D).
The patient underwent uniportal video-assisted thoracoscopic wedge resection of the right upper lobe with lymph node sampling. The surgical margins were negative. Gross examination revealed a well-circumscribed, gray-white solid nodule measuring 1.8×1.6×1.5 cm.
Histologic examination revealed a hypercellular spindle-cell sarcoma producing irregular, lace-like malignant osteoid directly rimmed and permeated by atypical cells; focal chondroid differentiation was also present (Figure 2A, 2B). IHC was performed to confirm the diagnosis and rule out other malignancies. The tumor cells showed strong diffuse nuclear positivity for SATB2, supporting osteoblastic differentiation. The Ki-67 proliferation index was approximately 30%. Tumor suppressor protein (p53) showed a diffuse strong nuclear staining pattern, suggestive of a mutant phenotype. Epithelial markers (low-molecular-weight cytokeratin antibody CK8/18 [CAM5.2], epithelial membrane antigen, pan-cytokeratin antibody) were largely negative. Markers for vascular tumors (CD34) and solitary fibrous tumor (signal transducer and activator of transcription 6 [STAT6]) were negative. Smooth muscle actin (SMA) and S100 showed focal positivity, while desmin was negative. B-cell lymphoma 2 (BCL-2) showed partial positivity (Figure 3A–3K). Although IHC for hepatocellular markers (eg, HepPar-1 and arginase-1) were not performed, the diagnosis of metastatic HCC was considered unlikely based on the following evidence: (1) serum alpha-fetoprotein levels remained within normal limits; (2) follow-up imaging showed no evidence of intrahepatic recurrence or extrahepatic metastasis; and (3) the histomorphology showed definitive malignant osteoid formation, which is not a feature of HCC. Correlation of morphology, immunophenotype, and whole-body imaging excluded an extrathoracic osteogenic primary and established a final diagnosis of PPOS.
To diagnose a lung mass as PPOS, the following criteria must be met: (1) the tumor must be composed entirely of homogeneous osteosarcoma tissue; (2) the tumor must be capable of producing osteoid or bone matrix; and (3) the tumor must originate from the lung and exclude the possibility of other primary osteogenic tumors [6]. The patient received 6 cycles of adjuvant therapy with liposomal doxorubicin combined with cisplatin, with no recurrence or metastasis observed during 9 months of follow-up. This regimen is consistent with contemporary sarcoma protocols; however, evidence specific to PPOS remains limited [1,3].
Discussion
This case highlights that PPOS can present as a small, well-circumscribed subpleural nodule, even in patients with a history of malignancy, and underscores the critical importance of a structured imaging-pathology workup to distinguish it from metastatic disease. In our patient with prior HCC, the initial clinical suspicion was pulmonary metastasis. However, the combination of normal serum alpha-fetoprotein level, absence of hepatic or extrahepatic recurrence on imaging, an IHC profile negative for epithelial, vascular, and solitary fibrous tumor markers, and the definitive histologic finding of malignant lace-like osteoid with SATB2 positivity collectively supported a diagnosis of PPOS.
PPOS is an extremely rare malignancy, which can be diagnosed in patients with a history of other cancers [1,3,7]. The differential diagnosis includes metastasis from osteosarcoma, primary lung carcinoma, and benign pulmonary lesions, such as hamartomas [3]. In this context, PET/CT and whole-body bone scintigraphy are invaluable tools for excluding an occult primary skeletal osteosarcoma [3,8], while IHC for SATB2 serves as a highly specific marker for confirming osteoblastic differentiation [9,10].
In our case, the tumor size of 1.7 cm was smaller than those typically reported, which are often larger than 5 cm [1,3]. This small tumor size likely contributed to the favorable prognosis observed in our patient [1]. Surgical resection is the standard treatment, and complete resection has been shown to improve outcomes [1,3]. Adjuvant doxorubicin-cisplatin regimens have been used in PPOS, although their benefit remains uncertain, given limited data [1,3]. Further research is needed to establish standardized diagnostic and therapeutic guidelines for PPOS and to validate the diagnostic and potential prognostic utility of markers like SATB2 [1,10].
Conclusions
This case illustrates the diagnostic complexity of PPOS in a patient with prior HCC. Small, well-circumscribed pulmonary nodules can harbor histologically malignant lesions, such as PPOS. Early surgical intervention within a structured imaging-pathology workup can achieve favorable short-term outcomes in selected patients with PPOS.
Figures
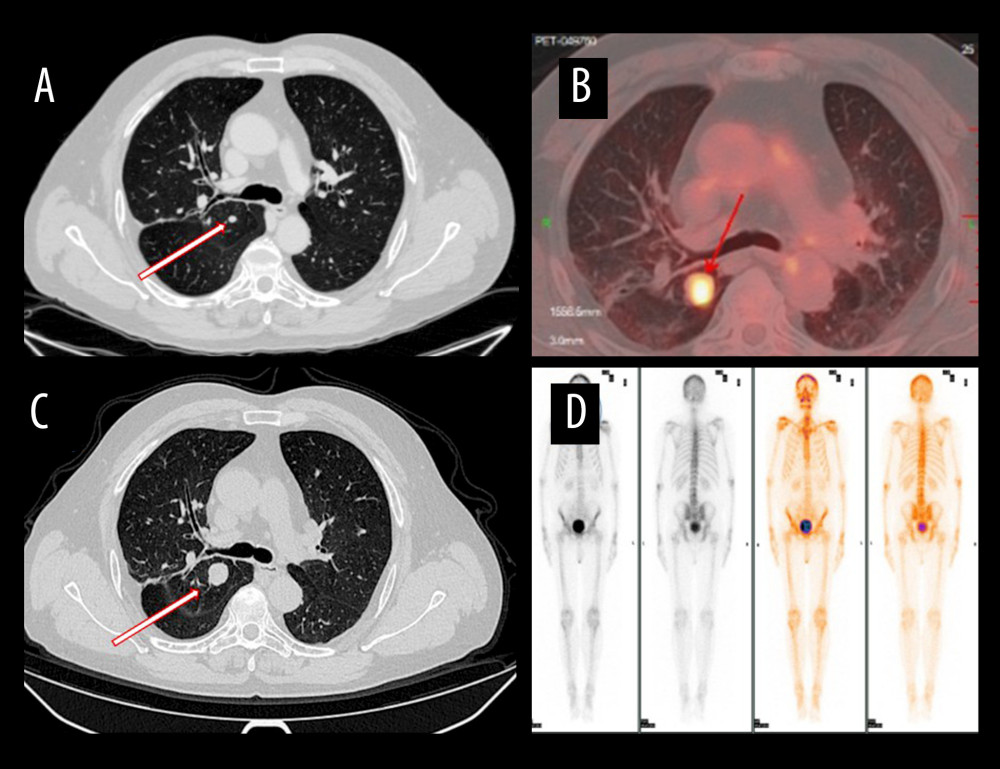 Figure 1. Chest imaging workup of the right upper lobe nodule(A) Computed tomography (CT) from August 2024 shows a 0.7-cm, smooth-edged subpleural nodule. (B) CT from January 2025 demonstrates interval growth to 1.7 cm. (C) Positron-emission tomography/CT reveals increased uptake (SUVmax 5.2). (D) Whole-body bone scintigraphy shows no skeletal uptake, providing evidence against a bone primary or osseous metastasis.
Figure 1. Chest imaging workup of the right upper lobe nodule(A) Computed tomography (CT) from August 2024 shows a 0.7-cm, smooth-edged subpleural nodule. (B) CT from January 2025 demonstrates interval growth to 1.7 cm. (C) Positron-emission tomography/CT reveals increased uptake (SUVmax 5.2). (D) Whole-body bone scintigraphy shows no skeletal uptake, providing evidence against a bone primary or osseous metastasis. 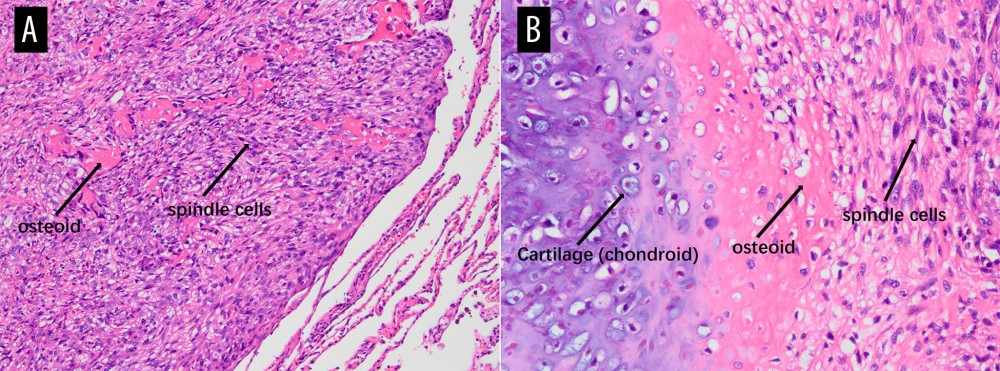 Figure 2. Histopathology of primary pulmonary osteosarcoma with hematoxylin and eosin staining(A) Magnification ×100. Low-power view of a hypercellular spindle-cell neoplasm within lung parenchyma, with irregular dense eosinophilic osteoid deposits (arrow named “osteoid”) rimmed and permeated by tumor cells (labeled “spindle cells”). Residual alveolar septa/fibrous stroma are present at the periphery, indicating adjacency to native lung. (B) Magnification ×200. Higher-power view demonstrates a triphasic pattern with focal chondroid differentiation (labeled “Cartilage, chondroid”) showing basophilic matrix containing lacunae with chondrocyte-like tumor cells, transitioning to abundant lace-like/trabecular eosinophilic osteoid (labeled “osteoid”). The osteoid is directly produced by and rimmed and permeated by atypical spindle tumor cells (labeled “spindle cells”), exhibiting nuclear pleomorphism, hyperchromasia, and frequent mitotic figures. The intimate association of malignant spindle cells with tumor osteoid, together with focal chondroid differentiation, supports an osteoid-forming high-grade sarcoma (osteoblastic osteosarcoma phenotype).
Figure 2. Histopathology of primary pulmonary osteosarcoma with hematoxylin and eosin staining(A) Magnification ×100. Low-power view of a hypercellular spindle-cell neoplasm within lung parenchyma, with irregular dense eosinophilic osteoid deposits (arrow named “osteoid”) rimmed and permeated by tumor cells (labeled “spindle cells”). Residual alveolar septa/fibrous stroma are present at the periphery, indicating adjacency to native lung. (B) Magnification ×200. Higher-power view demonstrates a triphasic pattern with focal chondroid differentiation (labeled “Cartilage, chondroid”) showing basophilic matrix containing lacunae with chondrocyte-like tumor cells, transitioning to abundant lace-like/trabecular eosinophilic osteoid (labeled “osteoid”). The osteoid is directly produced by and rimmed and permeated by atypical spindle tumor cells (labeled “spindle cells”), exhibiting nuclear pleomorphism, hyperchromasia, and frequent mitotic figures. The intimate association of malignant spindle cells with tumor osteoid, together with focal chondroid differentiation, supports an osteoid-forming high-grade sarcoma (osteoblastic osteosarcoma phenotype). 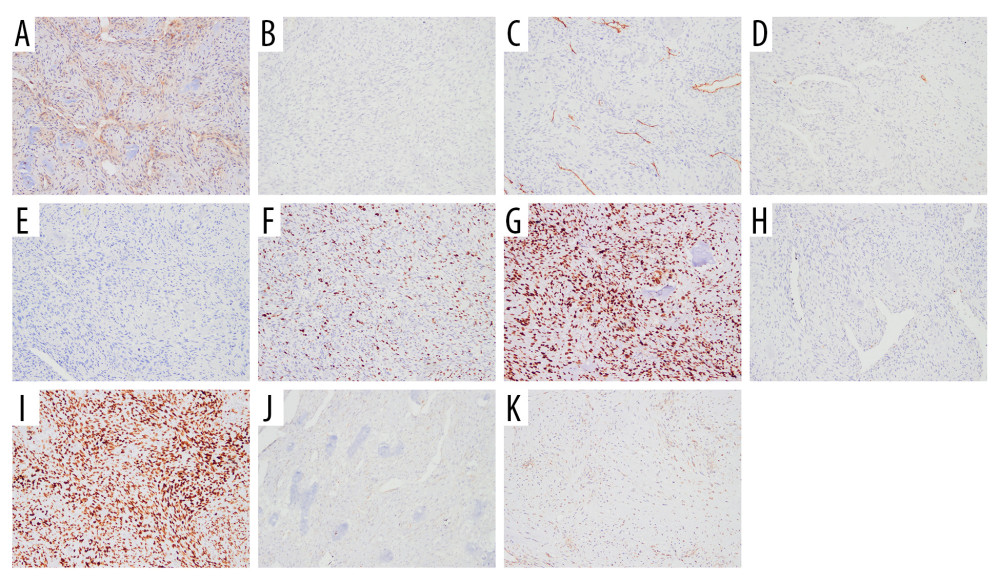 Figure 3. Immunohistochemical panel of the tumor (all with magnification ×100)(A) B-cell lymphoma 2 (BCL-2): focal positivity. (B) Low-molecular-weight cytokeratin antibody CK8/18 (CAM5.2): negative (rare weak-positive cells). (C) CD34: restricted to vascular endothelium (internal control). (D) Cytokeratin: negative (rare weak-positive cells). (E) Desmin: negative. (F) Ki-67 proliferation: approximately 30% labeling index. (G) Tumor suppressor protein (p53): diffuse strong nuclear staining (mutant-type pattern). (H) S100 protein family: focal positivity. (I) Special AT-rich sequence-binding protein 2 (SATB2): diffuse nuclear positivity. (J) Smooth muscle actin (SMA): focal positivity. (K) Signal transducer and activator of transcription 6 (STAT6): negative. Epithelial membrane antigen (not shown) was also negative. The overall IHC profile supports osteoblastic differentiation and argues against epithelial, vascular, and solitary fibrous tumor lineages.
Figure 3. Immunohistochemical panel of the tumor (all with magnification ×100)(A) B-cell lymphoma 2 (BCL-2): focal positivity. (B) Low-molecular-weight cytokeratin antibody CK8/18 (CAM5.2): negative (rare weak-positive cells). (C) CD34: restricted to vascular endothelium (internal control). (D) Cytokeratin: negative (rare weak-positive cells). (E) Desmin: negative. (F) Ki-67 proliferation: approximately 30% labeling index. (G) Tumor suppressor protein (p53): diffuse strong nuclear staining (mutant-type pattern). (H) S100 protein family: focal positivity. (I) Special AT-rich sequence-binding protein 2 (SATB2): diffuse nuclear positivity. (J) Smooth muscle actin (SMA): focal positivity. (K) Signal transducer and activator of transcription 6 (STAT6): negative. Epithelial membrane antigen (not shown) was also negative. The overall IHC profile supports osteoblastic differentiation and argues against epithelial, vascular, and solitary fibrous tumor lineages. References
1. Huang W, Deng HY, Li D, Characteristics and prognosis of primary pulmonary osteosarcoma: A pooled analysis: J Cardiothorac Surg, 2022; 17(1); 240
2. Nascimento AG, Unni KK, Bernatz PE, Sarcomas of the lung: Mayo Clin Proc, 1982; 57(6); 355-59
3. Wen X, Xue L, Jiang X, A 17-year-old male with primary pulmonary osteosarcoma: A case report: Front Med (Lausanne), 2024; 11; 1364937
4. Kadowaki T, Hamada H, Yokoyama A, Two cases of primary pulmonary osteosarcoma: Intern Med, 2005; 44(6); 632-37
5. Machado I, Navarro S, Picci P, Llombart-Bosch A, The utility of SATB2 immunohistochemical expression in distinguishing between osteosarcomas and their malignant bone tumor mimickers, such as Ewing sarcomas and chondrosarcomas: Pathol Res Pract, 2016; 212(9); 811-16
6. Zhai D, Cai W, Fan G, Case report: Primary extraskeletal osteosarcoma in the lung and pulmonary artery: Front Oncol, 2021; 11; 673494
7. Loose JH, el-Naggar AK, Ro JY, Primary osteosarcoma of the lung: Report of two cases and review of the literature: J Thorac Cardiovasc Surg, 1990; 100(6); 867-73
8. Oh C, Bishop MW, Cho SY, 18F-FDG PET/CT in the management of osteosarcoma: J Nucl Med, 2023; 64(6); 842-51
9. Conner JR, Hornick JL, SATB2 is a novel marker of osteoblastic differentiation in bone and soft tissue tumours: Histopathology, 2013; 63(1); 36-49
10. Warmke LM, Maloney N, Leung CH, SATB2 expression in undifferentiated pleomorphic sarcomas of bone: Am J Clin Pathol, 2022; 158(2); 235-41
Figures
Figure 1. Chest imaging workup of the right upper lobe nodule(A) Computed tomography (CT) from August 2024 shows a 0.7-cm, smooth-edged subpleural nodule. (B) CT from January 2025 demonstrates interval growth to 1.7 cm. (C) Positron-emission tomography/CT reveals increased uptake (SUVmax 5.2). (D) Whole-body bone scintigraphy shows no skeletal uptake, providing evidence against a bone primary or osseous metastasis.Figure 2. Histopathology of primary pulmonary osteosarcoma with hematoxylin and eosin staining(A) Magnification ×100. Low-power view of a hypercellular spindle-cell neoplasm within lung parenchyma, with irregular dense eosinophilic osteoid deposits (arrow named “osteoid”) rimmed and permeated by tumor cells (labeled “spindle cells”). Residual alveolar septa/fibrous stroma are present at the periphery, indicating adjacency to native lung. (B) Magnification ×200. Higher-power view demonstrates a triphasic pattern with focal chondroid differentiation (labeled “Cartilage, chondroid”) showing basophilic matrix containing lacunae with chondrocyte-like tumor cells, transitioning to abundant lace-like/trabecular eosinophilic osteoid (labeled “osteoid”). The osteoid is directly produced by and rimmed and permeated by atypical spindle tumor cells (labeled “spindle cells”), exhibiting nuclear pleomorphism, hyperchromasia, and frequent mitotic figures. The intimate association of malignant spindle cells with tumor osteoid, together with focal chondroid differentiation, supports an osteoid-forming high-grade sarcoma (osteoblastic osteosarcoma phenotype).Figure 3. Immunohistochemical panel of the tumor (all with magnification ×100)(A) B-cell lymphoma 2 (BCL-2): focal positivity. (B) Low-molecular-weight cytokeratin antibody CK8/18 (CAM5.2): negative (rare weak-positive cells). (C) CD34: restricted to vascular endothelium (internal control). (D) Cytokeratin: negative (rare weak-positive cells). (E) Desmin: negative. (F) Ki-67 proliferation: approximately 30% labeling index. (G) Tumor suppressor protein (p53): diffuse strong nuclear staining (mutant-type pattern). (H) S100 protein family: focal positivity. (I) Special AT-rich sequence-binding protein 2 (SATB2): diffuse nuclear positivity. (J) Smooth muscle actin (SMA): focal positivity. (K) Signal transducer and activator of transcription 6 (STAT6): negative. Epithelial membrane antigen (not shown) was also negative. The overall IHC profile supports osteoblastic differentiation and argues against epithelial, vascular, and solitary fibrous tumor lineages. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133