16 December 2025: Articles 
Electronic Gastroscopy in Identifying Hidden Tonsillar Foreign Bodies: A Case of a Completely Embedded Sunflower Seed Shell
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Educational Purpose (only if useful for a systematic review or synthesis)
Deng LiangDOI: 10.12659/AJCR.949052
Am J Case Rep 2025; 26:e949052






Abstract
BACKGROUND: Pharyngeal foreign bodies are common in otolaryngology and often occur as isolated events. Swallowing can cause the foreign body to shift, making detection by laryngoscopy difficult. Delayed diagnosis and treatment may result in complications such as cervical masses, floor of mouth abscesses, retropharyngeal abscesses, laryngeal granulomas, or tongue masses. Penetration of a foreign body into the tonsil can lead to recurrent unilateral tonsillitis. For foreign bodies undetectable by laryngoscopy, digestive endoscopy may provide valuable diagnostic assistance.
CASE REPORT: On June 1, 2024, a 38-year-old woman presented with throat pain and persistent foreign body sensation after consuming sunflower seeds. She underwent 2 otolaryngologic examinations, but no foreign body was detected by laryngoscopy, and her symptoms persisted. On June 3, she underwent gastroscopy under intravenous general anesthesia. A yellow dot was observed on the right palatal tonsil, suggesting a completely embedded foreign body. Using foreign body forceps, a 4-mm wooden fibrous fragment was extracted. The patient experienced immediate relief; her throat pain and foreign body sensation completely resolved after removal.
CONCLUSIONS: When a foreign body cannot be identified by laryngoscopy, it may have completely penetrated the tonsil. In such cases, electronic gastroscopy can serve as a valuable adjunct in the diagnosis and management of pharyngeal foreign bodies.
Keywords: Foreign Bodies, Gastroscopes, tonsillitis, Humans, Female, adult, Gastroscopy, Palatine Tonsil, Helianthus, Seeds
Introduction
Pharyngeal foreign bodies are mainly detected via laryngoscopy. Sunflower seed shells are a common type of pharyngeal foreign body, but complete penetration of the tonsil is rare and easily misdiagnosed. In cases where laryngoscopy fails to detect a foreign body, electronic gastroscopy may provide diagnostic assistance. The following report describes a case in which a pharyngeal foreign body was identified through electronic gastroscopy.
Case Report
A 38-year-old woman experienced throat pain and foreign body sensation after consuming sunflower seeds; she sought treatment at the otolaryngology department on June 1, 2024. Although no foreign body was detected by laryngoscopy, the symptoms persisted. On the afternoon of June 2, she returned for reevaluation, and a repeat examination did not show any foreign body. Apart from throat pain, her overall health was good; she had no fever, no cervical lymphadenopathy, and normal pulse, respiration, and blood pressure. The otolaryngologist considered the possibility of pharyngitis or mucosal abrasion and prescribed acetaminophen (0.5 g per dose, twice daily). However, the treatment did not alleviate her symptoms. By the morning of June 3, the throat pain had worsened, and the patient requested further investigation via gastroscopy. Thus, gastroscopy was performed under intravenous general anesthesia (propofol 500 mg per vial, administered by continuous intravenous infusion [40 mg/10 s]), limited to examination of the throat without exploration of the upper digestive tract. The oropharynx and laryngopharynx were meticulously examined using a transparent cap attached to the endoscope, but no obvious foreign body was observed. After cap removal and lens cleaning, a second examination revealed no abnormalities in the epiglottis or the left and right pyriform fossae. When the endoscope was retracted to the tongue root, a yellow dot approximately 1 mm in diameter was noted on the surface of the right palatal tonsil, suggesting an embedded foreign body. Using foreign body forceps, a yellow fibrous fragment approximately 4 mm in length was successfully extracted. Subsequent examination confirmed that the yellow dot had disappeared and that the tonsillar surface was intact, without evidence of bleeding or purulent discharge (Figures 1, 2). After removal, the patient’s symptoms – including throat pain and foreign body sensation – completely resolved.
Discussion
Pharyngeal foreign bodies are a common emergency in otorhinolaryngology-head and neck surgery, most commonly found in the tonsils, tongue root, epiglottic vallecula, and pyriform fossa [1]. In most cases, foreign bodies can be detected by direct visualization or with specialized instruments such as indirect or fiberoptic laryngoscopy, enabling straightforward identification and removal by the otorhinolaryngologist.
The surface of each tonsil contains multiple crypts that can easily trap foreign material. When a foreign body is forcibly swallowed, it may become completely embedded within the tonsillar tissue, rendering it invisible on the tonsillar surface. Consistent with this mechanism, a previous report described sewing needles embedded in the tonsils [2]. In a large retrospective analysis of 829 pediatric cases of foreign bodies in the ear, nose, and throat, the most frequently affected sites were the nose (58.7%) and ear (20.2%), followed by the mouth, pharynx, or tonsil (12.3%); esophagus (6.2%); and tracheobronchial tree (2.4%). The most common types of foreign bodies identified at each site were beads in the nose (30.8%); beads in the ear (32.1%); fish bones in the mouth, pharynx, or tonsil (56.8%); nuts and peanuts in the tracheobronchial tree (70%); and coins or disc batteries in the esophagus (80.7%) [3]. Moreover, sunflower seeds are among the most common aspirated airway foreign bodies in children [4]. Nevertheless, there have been no documented cases of pharyngeal foreign bodies caused by sunflower seed shells.
A previously reported case of a tonsillar foreign body bears similarity to the present case. A 12-year-old girl sustained a tonsillar injury from a ballpoint pen cap, resulting in laceration over the left tonsil. Although antibiotic treatment temporarily relieved her symptoms, the pain recurred. Upon careful examination, a piece of embedded plastic was identified in the upper pole of the left tonsil, surrounded by an area of inflammation. Under general anesthesia, the bottom plug of a ballpoint pen was successfully removed from the tonsil. The previous case supports the possibility that completely embedded tonsillar foreign bodies may escape initial diagnosis [5].
A unique aspect of the present case is that the patient had a clear history of consuming sunflower seed shells and experienced throat pain while eating them. Although no foreign body was identified during 2 otolaryngology consultations and repeated laryngoscopic examinations, the patient continued to report persistent throat pain, discomfort, and foreign body sensation. This prompted a gastroscopic examination using a transparent cap to enhance observation of the pharyngeal structures. Initially, no foreign body was detected, but during endoscope retraction, a small yellow dot was observed on the surface of the right palatal tonsil. We speculated that the foreign body had completely penetrated the tonsil and that the yellow dot represented either inflammation or the foreign body itself. Using foreign body forceps, the site was carefully explored; we confirmed that the yellow dot was a penetrating fiber from a sunflower seed shell. This case underscores the potential risk of overlooking small or atypical findings. If the tonsils are not examined thoroughly during gastroscopy, or if such findings are misinterpreted as simple inflammation, a penetrated sunflower seed shell may lead to a tonsillar abscess. The key conclusion from this case is that when a patient has a clear history of foreign body ingestion and continues to experience pain or a persistent foreign body sensation, multiple negative nasopharyngeal or endoscopic examinations cannot definitively exclude foreign body retention. Unless all possible causes are excluded, symptoms should not be attributed solely to mucosal inflammation from prior injury. Clinicians should consider the possibility of complete mucosal penetration and carefully inspect all areas of the pharynx, including the tonsils, during endoscopic examination. Any suspicious finding should receive a high index of suspicion and be further explored using foreign body forceps when feasible. This approach may help reduce the risk of foreign body retention and associated complications. An increasing number of early-stage pharyngeal cancers have been detected via electronic gastroscopy, possibly because the high image clarity enables identification of subtle manifestations of hypopharyngeal cancer. Thus, for concealed foreign bodies in the pharynx, electronic gastroscopy – with its clear field of view – can aid in detecting retained foreign material [6]. Similar to the present case, Koito et al. reported an instance in which a fish bone was completely embedded beneath the esophageal mucosa and successfully removed through endoscopic mucosal incision [7]. These examples demonstrate that an endoscope with a clear field of view can serve as an adjunct for detecting and removing completely embedded foreign bodies.
Conclusions
In our case, no foreign body was identified during laryngoscopy because the object had completely penetrated the tonsil. Electronic gastroscopy aided in the detection and management of pharyngeal foreign bodies.
Figures
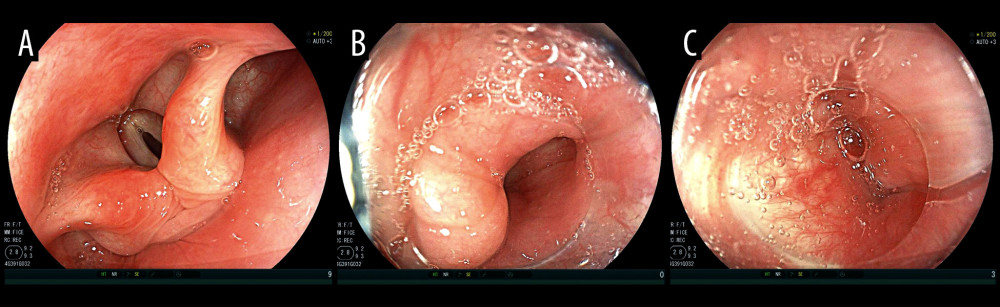 Figure 1. (A) Panoramic view of the pharynx, no foreign bodies detected. (B) Right pyriform fossa, no foreign bodies detected. (C) Left pyriform fossa, no foreign bodies detected.
Figure 1. (A) Panoramic view of the pharynx, no foreign bodies detected. (B) Right pyriform fossa, no foreign bodies detected. (C) Left pyriform fossa, no foreign bodies detected. 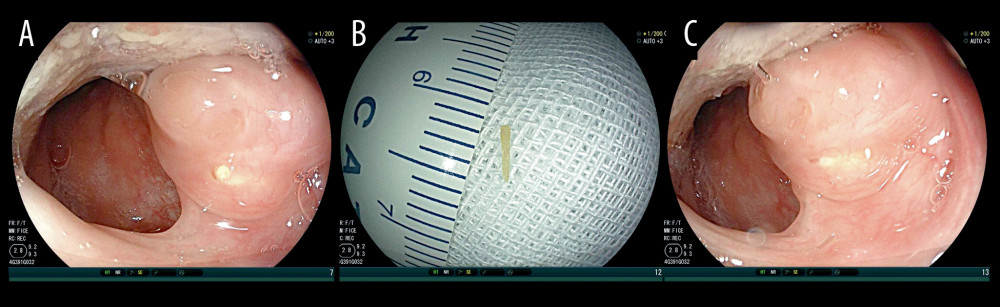 Figure 2. (A) A yellow dot approximately 0.5 mm in diameter on the surface of the right palatal tonsil. (B) A wooden fibrous foreign body measuring 3 mm in length removed from yellow dot on the right palatal tonsil. (C) Disappearance of the yellow dot after removal of the foreign body from the right palatal tonsil.
Figure 2. (A) A yellow dot approximately 0.5 mm in diameter on the surface of the right palatal tonsil. (B) A wooden fibrous foreign body measuring 3 mm in length removed from yellow dot on the right palatal tonsil. (C) Disappearance of the yellow dot after removal of the foreign body from the right palatal tonsil. References
1. Chen H, Wu C, Zhang Z, Migratory pharyngeal foreign bodies and related complications: Analysis of 20 cases: Am J Otolaryngol, 2022; 43(2); 103390
2. Arora S, Sharma JK, Pippal SK, An unusual foreign body (sewing needle tip) in the tonsils: Braz J Otorhinolaryngol, 2009; 75(6); 908
3. Loperfido A, Mammarella F, Giorgione C, Management of foreign bodies in the ear, nose and throat in pediatric patients: Real-life experience in a large tertiary hospital: Cureus, 2022; 14(10); e30739
4. Özdemir C, Sökücü SN, Karasulu L, Foreign body aspiration in adult: Analysis of 28 cases: Eurasian J Pulmonol, 2015; 17; 29-34
5. Sekhar P, El-Jassar P, Ell SR, Recurrent unilateral tonsillitis secondary to a penetrating foreign body in the tonsil: J Laryngol Otol, 1998; 112(6); 584
6. Ni XG, Zhang QQ, Zhu JQ, Wang GQ, Hypopharyngeal cancer associated with synchronous oesophageal cancer: Risk factors and benefits of image-enhanced endoscopic screening: J Laryngol Otol, 2018; 132(2); 154-61
7. Koito Y, Asano T, Matsumoto S, Mashima H, Endoscopic mucosal incision to remove a fish bone completely embedded under the esophageal mucosa: A case report and literature review: Am J Case Rep, 2022; 23; e936773
Figures
Figure 1. (A) Panoramic view of the pharynx, no foreign bodies detected. (B) Right pyriform fossa, no foreign bodies detected. (C) Left pyriform fossa, no foreign bodies detected.Figure 2. (A) A yellow dot approximately 0.5 mm in diameter on the surface of the right palatal tonsil. (B) A wooden fibrous foreign body measuring 3 mm in length removed from yellow dot on the right palatal tonsil. (C) Disappearance of the yellow dot after removal of the foreign body from the right palatal tonsil. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133