23 December 2025: Articles 
Low-Grade Appendiceal Mucinous Neoplasm as an Incidental Finding During Cesarean Section: A Case Report
Challenging differential diagnosis, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Vesna PaunovicDOI: 10.12659/AJCR.949554
Am J Case Rep 2025; 26:e949554






Abstract
BACKGROUND: Appendiceal mucinous neoplasm (AMN) is a rare tumor, representing 0.2-0.7% of all appendiceal neoplasms. Low-grade AMN (LAMN) occurs more often in women and is often misdiagnosed as appendicitis due to its vague symptoms. It involves mucin accumulation causing appendiceal dilation and carries a risk of pseudomyxoma peritonei (PMP). Prognosis depends on disease extent, with survival rates declining once the tumor spreads beyond the appendix. During pregnancy, diagnosis is challenging because of non-specific symptoms and limited imaging options, highlighting the importance of clinical vigilance and thorough intraoperative evaluation to ensure timely diagnosis and management.
CASE REPORT: This report describes the case of a 45-year-old woman with LAMN, incidentally discovered during an elective cesarean section at 40 weeks of gestation, and is the first documented report of this type in Serbia. The patient was asymptomatic, with unremarkable prenatal screenings. Intraoperative inspection revealed approximately 400 ml of thick gelatinous material (PMP) in the abdominal cavity and a tumor-like mass on the appendix. Following the initial appendectomy and biopsy, confirmed LAMN and elevated CA125 led to a secondary operation: extended right hemicolectomy and total omentectomy. This procedure confirmed mucin dissemination, highlighting the urgent need for oncologic intervention despite the tumor’s low grade.
CONCLUSIONS: Incidental discovery of LAMN during a cesarean section is extremely rare. This case demonstrates the need for intraoperative vigilance, thorough abdominal assessment, and multidisciplinary management to ensure accurate diagnosis and optimal outcomes for both mother and neonate in such complex situations.
Keywords: 17-alpha-Hydroxyprogesterone, Cesarean Section, Meditation, Operating Room Technicians, Pregnancy, Humans, Female, Appendiceal Neoplasms, Incidental Findings, Middle Aged, Adenocarcinoma, Mucinous, Pregnancy Complications, Neoplastic, Appendectomy
Introduction
Appendiceal mucinous neoplasm (AMN) is a rare condition, constituting 0.2% to 0.7% of all appendiceal neoplasms [1–3]. Research indicates that LAMN is more common in women, accounting for 88% of cases, with a female-to-male ratio of 4: 1 [4,5]. Its incidence is low but has increased in various countries worldwide [4,5]. Globally, it varies between 0.2% and 2.5% [5–7], with rates of 0.07% to 0.8% in Chile [4], 0.78% in Turkey [8], 0.9% in Spain [9,10], 0.9% to 1.7% in the United States [11], 1.24% in Finland [7], 2.3% in Japan [4], and <3% in Tunisia [12].
Mucinous tumors of the bowel, ovaries, and appendix can be benign or have low-grade malignant potential. Histological diagnosis is required to identify the origin and grade of the tumor, and careful surgical excision is necessary to avoid the complication of pseudomyxoma peritonei. Because mucinous tumors are an uncommon cause of acute abdomen, they are frequently initially misdiagnosed as acute appendicitis. In 0.7% to 7% of appendectomies performed for suspected appendicitis, an epithelial tumor of the appendix is unexpectedly discovered upon histological examination [13]. The lumen of the appendix is dilated due to the accumulation of mucinous substance [4–7]. These tumors cause cystic dilation of the appendix through the accumulation of mucus in the lumen and can spread to the peritoneum, resulting in a specific syndrome known as pseudomyxoma peritonei (PMP), which is often progressive and fatal. Since both histologically benign and malignant AMNs can spread to the peritoneal cavity as PMP, a definitive diagnosis, including pathology and appropriate treatment, is crucial for AMN. Previously published case reports describe only a few similar cases of LAMN diagnosed during pregnancy. These reports highlight the diagnostic challenges and the importance of intraoperative recognition of unusual appendiceal pathology.
This report describes the case of a 45-year-old woman with a low-grade appendiceal mucinous neoplasm (LAMN) as an incidental finding during cesarean section, representing the first documented case of this type in Serbia.
Case Report
A 45-year-old woman (gravida 0, para 0) achieved pregnancy through her seventh in vitro fertilization (IVF) cycle following a diagnostic hysteroscopy performed in 2018. She had a comorbidity of hypothyroidism. An early pregnancy ultrasound revealed no abnormalities, with physiological fetal development. During the pregnancy, due to high risk, she received treatment including 250 mg of intramuscular progesterone on day 3, 100 mg of vaginal Utrogestan, 2 mg of Estrofem 3 times daily, 0.2 ml of Clenax subcutaneously once daily, 5 mg of prednisone once daily, 40 mg of Controlok once daily, 100 mg of aspirin once daily, 800 mcg of Folnic once daily, 100 mg of vitamin E, and 100 mg of vitamin C.
At 40 weeks of gestation, she underwent an elective cesarean section. A female newborn, weighing 3780 g and measuring 55 cm, was born without complications, with Apgar scores 9 and 10 at 1 and 5 minutes, respectively. During the intraoperative inspection, no abnormalities in the uterus or adnexa were found. However, approximately 400 ml of thick gelatinous material was discovered in the abdominal cavity, consistent with pseudomyxoma peritonei (PMP), and it sent for cytological and histopathological analysis.
The uterus was appropriately sized for the gestation period. Both adnexa were hypertrophied but free of lesions. The appendix was elongated, with a tumefaction measuring 2–3 cm at its tip, yellowish-white in appearance. After the fetus was delivered, appendectomy and biopsy of the omentum were performed. An abdominal drain was placed in the pouch of Douglas, and all specimens were sent for histopathological analysis.
Preoperative routine laboratory tests along with standard prenatal sonography showed no abnormalities. Importantly, the patient presented no preoperative symptoms suggestive of appendicitis.
Histopathological examination confirmed low-grade appendiceal mucinous neoplasm (LAMN) (Figure 1). The tumor was confined to the appendix, but tumor tissue was found at the resection margin. Cytology revealed reactively changed mesothelial cells, inflammatory cells, and abundant basophilic material. On the sixth postoperative day, a CT scan of the abdomen and pelvis was performed. The findings showed a right iliac abscess (7.5×10 cm), in proximity to the cecum and ascending colon, with fluid-gas content, but no metastases or invasion. The tumor marker cancer antigen 125 (CA125) measured on the 11th postoperative day was elevated (103.9 U/ml). A colorectal surgeon was consulted, and a multidisciplinary team decided to perform a secondary surgery due to the risk of peritoneal dissemination. Exploratory laparotomy revealed a tumor mass in the cecum (3×2 cm) with an abscess. Extended right hemicolectomy with ileocolic anastomosis and total omentectomy were performed. Histopathology confirmed LAMN with rupture and dissemination of acellular mucin across the omentum and the serosa of the intestines, while cellular mucin was detected on the appendix serosa and in the gelatinous peritoneal material (Figure 2). Fifteen lymph nodes were isolated, all showing reactive changes without metastases.
The chronological reporting of surgical findings and postoperative interventions is essential for understanding the diagnostic and therapeutic challenges in this case. This case emphasizes the importance of intraoperative vigilance and timely decision-making in managing incidental pathology findings.
Discussion
LAMN is an uncommon appendiceal pathology [14], with only a few prior reports of LAMN during pregnancy [15]. LAMNs are tumors found in the appendix or the adjacent mucosal wall of the cecum [16,17]. These tumors characteristically cause cystic dilation of the appendix due to the accumulation of abundant gelatinous material in the lumen. They can spread throughout the peritoneal cavity in the form of gelatinous deposits known as pseudomyxoma peritonei (PMP) [4]. While PMP is not locally invasive, the mucin causes local destruction, and the ensuing fibrosis and obstruction can result in complications [18–20]. When restricted to the appendix, AMNs are slow-growing lesions with a 96% 5-year disease-free survival rate. However, if AMNs extend beyond the appendix, the disease-free survival rate drops to 66% to 67% [1]. Therefore, early detection of AMN and appropriate treatment are crucial for prognosis [18,19,21–23]. Studies have found that patients with complete cytoreduction and pathological adenomyxoma had a 5-year survival rate of 86%, while those with incomplete cytoreduction had a 5-year survival rate of 20%. Tumors limited to the mucosa of the appendix can be cured through appendectomy, whereas any growth of neoplastic epithelium beyond the mucosa puts the patient at risk for peritoneal dissemination, adenocarcinoma, or PMP [19]. In our case, there was a rupture of the tumor capsule and leakage of mucinous content. PMP was also observed.
To the best of our knowledge, no cases of LAMN have been recorded in Serbia; research indicates that only a limited number of cases of LAMN during pregnancy have been reported previously. Inubashiri et al (2020) described an incidental finding of LAMN during cesarean section [15]. In addition, several other reports documented similar findings, including mucinous adenoma and mucinous adenocarcinoma of the appendix diagnosed during pregnancy-related procedures [21–23]. Four patients underwent laparotomy for acute abdomen during pregnancy, and mucinous adenocarcinoma was diagnosed in all cases. In 2 other asymptomatic patients, a right adnexal mass was incidentally found on obstetric ultrasound during the second trimester, leading to surgery. Of these 2 patients, one was diagnosed with mucinous adenocarcinoma of the appendix, while the other had a mucinous adenoma of the appendix with PMP. Both tumors were discovered incidentally during cesarean section, with mucinous adenocarcinoma confirmed in each case [22,23]. Our case was diagnosed during cesarean section, with histological findings confirming the tumor as LAMN with PMP.
Clinical manifestations of LAMN without PMP may include right lower-quadrant abdominal pain, a palpable mass, nausea, vomiting, gastrointestinal bleeding, and signs of intestinal intussusception [18,20]. The differential diagnosis for lower right abdominal pain includes a variety of conditions, such as appendicitis, appendiceal abscess, hydrosalpinx, ovarian tumors, endometriotic cysts, and enterocolitis in women. It is important to note that obstetric symptoms (eg, uterine contractions) can mask the clinical signs of appendiceal lesions in pregnant women [24]. Studies on AMN in pregnant women suggest that clinical manifestations, such as acute abdomen, may be indicative of cancer. Taken together, these findings highlight the significant challenges in the preoperative diagnosis of AMN during pregnancy. This is further supported by the findings of Villa et al, who reported the co-occurrence of LAMN with neuroendocrine tumors, underscoring the histopathological complexity and diagnostic difficulties of such neoplasms during surgical interventions [25].
Diagnosing and staging AMN can be challenging during pregnancy due to the limited availability of safe diagnostic methods and the non-specific clinical presentation. Pregnancy introduces unique diagnostic and therapeutic challenges when dealing with LAMN. The non-specific clinical presentation, physiological changes in the abdomen, and the limited use of radiological imaging due to fetal safety concerns can delay diagnosis or result in incidental findings during obstetric procedures. In this case, the absence of preoperative symptoms and the inability to perform preoperative abdominal CT or MRI highlights the importance of vigilance during obstetric surgery. The choice of surgical approach must balance maternal and fetal safety with oncologic principles, which requires interdisciplinary collaboration. Low-grade mucinous neoplasia is a rare condition, and its occurrence during pregnancy is even more uncommon [21,26].
LAMN is more common and has a higher likelihood of malignant association in women, making it an entity that ultrasound practitioners in gynecology should be familiar with. Computed tomography (CT) and magnetic resonance imaging (MRI) are useful in the preoperative diagnosis of AMN. Pregnancy increases the complexity of diagnosis and treatment. CT and MRI pose potential risks to the fetus, limiting their use. MRI of the abdomen and pelvis without contrast is a safe and informative alternative to CT during pregnancy for clarifying the diagnosis of peritoneal lesions [27]. CT of the abdomen can identify LAMN if the lumen of the appendix is greater than 1.3 cm and if cystic dilation and mural calcification are present. CT can also help differentiate between benign and malignant causes [28]. Ultrasound is considered a safe examination for pregnant women, but pregnancy can complicate both transabdominal and transvaginal ultrasound examinations in detecting appendiceal lesions, depending on gestational age [29]. Ileocecal region diseases (eg, ovarian cysts) are much more common in women than AMN; therefore, in many cases, AMN is diagnosed postoperatively rather than preoperatively. If the diagnosis is not made incidentally during routine ultrasound, it may be established during acute cases of peritonitis and appendicitis in pregnancy or intraoperatively during gynecological procedures for the removal of a suspicious adnexal mass [30]. In the largest series of surgical cases of LAMN (135 cases over 24 years), only 19% of patients had an accurate preoperative diagnosis, and only 2 were identified via ultrasound [31].
Another potential method for detecting AMN is through tumor markers. Specifically, markers like carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA 19-9), and cancer antigen 125 (CA125) are known to be elevated in AMN and may show slight fluctuations even during pregnancy [32]. A newly recognized sensitive marker for colorectal adenocarcinomas is SATB2 (Special AT-rich sequence-binding protein 2) [31]. Therefore, these markers could be valuable in making preoperative diagnoses as well as in monitoring progression and recurrence [33,34]. In our case, CA125 measured on the eleventh postoperative day showed elevated levels.
A recent study indicated that LAMN can be classified into 2 groups: one confined to the lumen of the appendix, and the other involving mucin and/or neoplastic epithelium in the submucosa, wall, and/or peri-appendicular tissue of the appendix, with or without perforation. The authors concluded that the latter subtype carries a higher risk of progression and should be managed with cytoreductive surgery and chemotherapy [3]. A population study in the Netherlands on benign AMN found an association with PMP in 2% of cases [3]. Taken together, these findings suggest that even benign LAMN may require careful monitoring. For AMN, aggressive treatment, including optimal debulking surgery and/or chemotherapy, is essential [4–8].
To our knowledge, there are no reports of preoperatively diagnosed AMN during pregnancy [22,23]. Further studies dedicated to understanding mucinous neoplasms may assist in designing a more targeted therapeutic plan for such patients. For pregnant women with slow or moderate disease progression, pregnancy (or the desire for pregnancy) should be allowed to continue until vaginal delivery. In patients with rapid progression, termination of pregnancy and definitive treatment may be necessary to protect the mother [22]. In our case, LAMN did not compromise the pregnancy, which proceeded without complications, and the woman delivered a term, healthy newborn via cesarean section.
Surgical resection of the appendix is often sufficient. Right hemicolectomy is frequently performed for mucinous cystadenocarcinoma, while appendectomy is sufficient for benign pathologies such as hyperplasia and cystadenoma.
Conclusions
The described case of a low-grade appendiceal mucinous neoplasm (LAMN), discovered incidentally during cesarean section, represents an exceptionally rare occurrence, particularly in pregnancy. Although the patient was asymptomatic and the lesion was detected unexpectedly, timely diagnosis and surgical intervention were crucial for a favorable outcome. This case emphasizes the importance of careful intraoperative assessment of abdominal and pelvic organs during obstetric procedures, as well as the need for multidisciplinary management to ensure optimal maternal and neonatal outcomes. Furthermore, it highlights the diagnostic challenges of mucinous neoplasms in pregnancy, where non-specific symptoms and limited imaging options can delay recognition.
Future studies and multicenter reports are warranted to better define diagnostic pathways, therapeutic strategies, and long-term maternal and neonatal outcomes in cases of incidentally discovered LAMN during pregnancy.
Figures
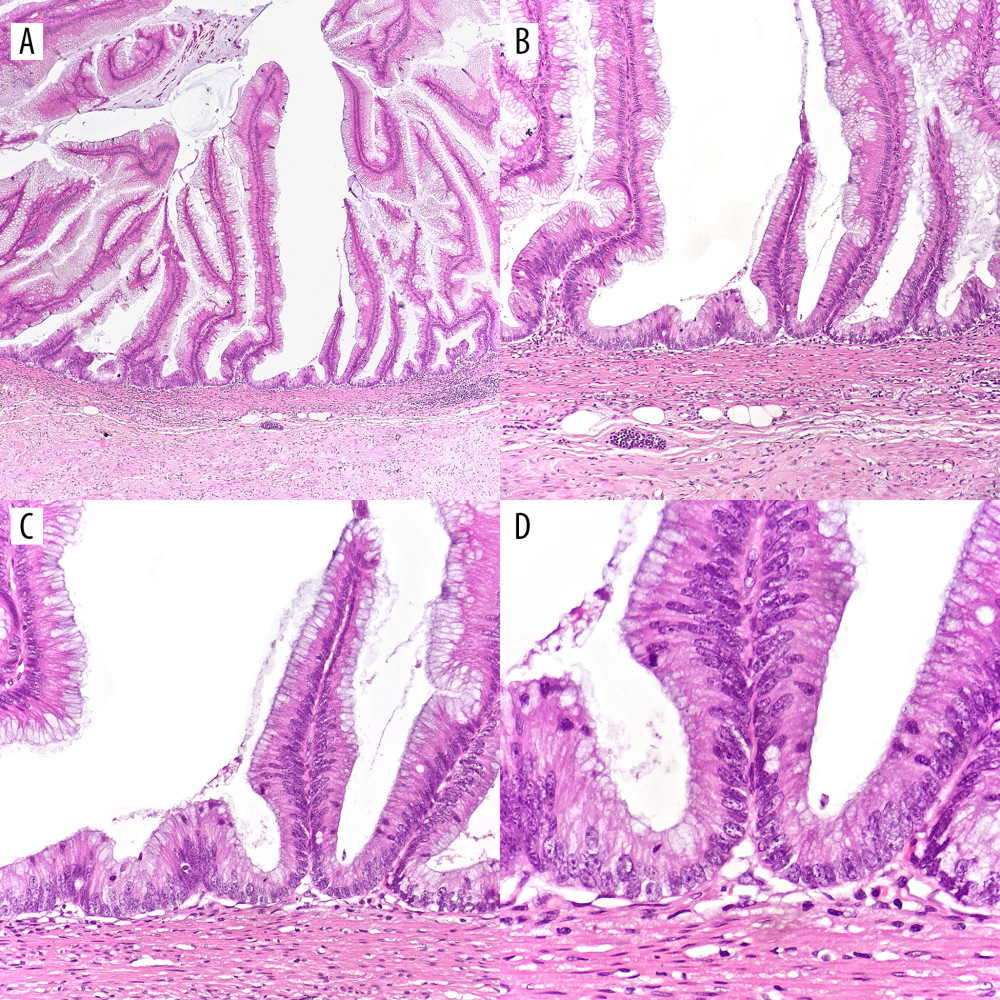 Figure 1. (A–D) Low-grade appendiceal mucinous neoplasm (LAMN). (A–C) Proliferation of mucinous epithelial cells forming villous structures within the appendiceal lumen. The underlying lymphoid tissue is atrophic, and the muscularis mucosae is effaced. Subepithelial fibrosis is present, and the lesion demonstrates a pushing (non-infiltrative) growth pattern. (D) The lesional epithelium shows abundant apical mucin and elongated nuclei with mild (low-grade) cytologic atypia. (H&E; magnifications: A ×40; B ×100; C ×200; D ×400).
Figure 1. (A–D) Low-grade appendiceal mucinous neoplasm (LAMN). (A–C) Proliferation of mucinous epithelial cells forming villous structures within the appendiceal lumen. The underlying lymphoid tissue is atrophic, and the muscularis mucosae is effaced. Subepithelial fibrosis is present, and the lesion demonstrates a pushing (non-infiltrative) growth pattern. (D) The lesional epithelium shows abundant apical mucin and elongated nuclei with mild (low-grade) cytologic atypia. (H&E; magnifications: A ×40; B ×100; C ×200; D ×400). 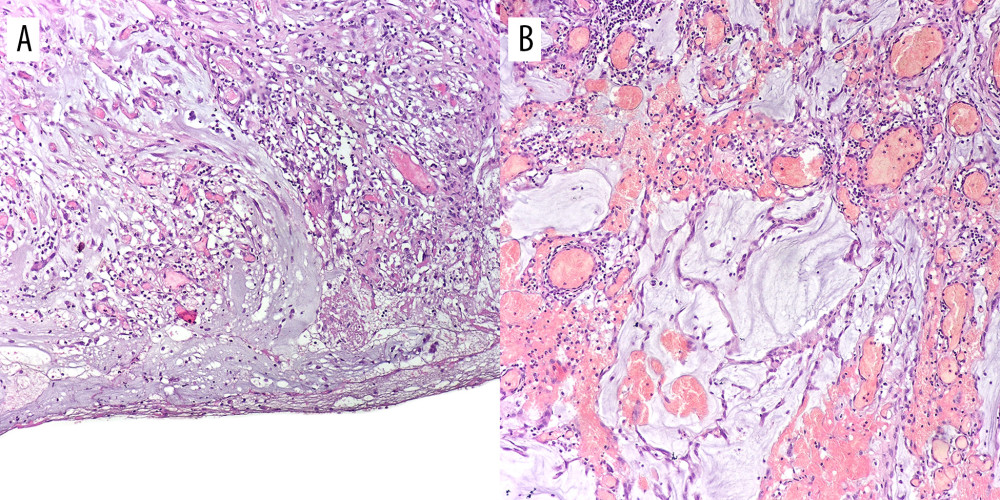 Figure 2. (A, B) Extruded mucin. (A) Mucin pools covering the serosa with a prominent granulation tissue response. (B) Extruded mucin surrounded by granulation tissue composed of fibroblasts, blood vessels and inflammatory cells. (H&E; magnifications: ×100).
Figure 2. (A, B) Extruded mucin. (A) Mucin pools covering the serosa with a prominent granulation tissue response. (B) Extruded mucin surrounded by granulation tissue composed of fibroblasts, blood vessels and inflammatory cells. (H&E; magnifications: ×100). References
1. Saleem N, Shahid F, Ali SM, Incidental low grade mucinous neoplasm of appendix in pregnancy: A case report & literature review: Ann Med Surg (Lond), 2020; 59; 195-98
2. Núñez-Rocha RE, Girón F, Rodríguez L, Incidence of appendiceal neoplasms in appendectomy patients: BMC Surg, 2023; 23(1); 287
3. Xiao J, Li P, Liu W, Analysis of clinical characteristics of low-grade appendiceal mucinous neoplasm (LAMN): A retrospective cohort study of 51 LAMN patients: J Investig Surg, 2020; 34(7); 721-27
4. Tajima T, Tajiri T, Mukai M, Single-center analysis of appendiceal neoplasms: Oncol Lett, 2018; 15(5); 6393-99
5. Turaga KK, Pappas SG, Gamblin TC, Importance of histologic subtype in the staging of appendiceal tumors: Ann Surg Oncol, 2012; 19(5); 1379-85
6. Beltrán MA, Tapia R, Madariaga JMalignant tumors of the cecal appendix in patients undergoing surgery for appendicitis in Region IV of Chile: Rev Chil Cir, 2013; 65(6); 509-14 [in Spanish]
7. Lietzén E, Grönroos JM, Mecklin JP, Appendiceal neoplasm risk associated with complicated acute appendicitis: A population-based study: Int J Colorectal Dis, 2019; 34(1); 39-46
8. Zhang Y, Zulfiqar M, Bluth MH, Molecular diagnostics in the neoplasms of small intestine and appendix: 2018 update: Clin Lab Med, 2018; 38(2); 343-55
9. Kunduz E, Bektasoglu HK, Unver N, Analysis of appendiceal neoplasms on 3544 appendectomy specimens for acute appendicitis: Retrospective cohort study of a single institution: Med Sci Monit, 2018; 24; 4421-26
10. Nutu OA, Marcacuzco Quinto AA, Manrique Municio AMucinous tumors of the appendix: Incidence, diagnosis and surgical treatment: Cir Esp, 2017; 95(6); 321-27 [in Spanish]
11. Loftus TJ, Raymond SL, Sarosi GA, Predicting appendiceal tumors among patients with appendicitis: J Trauma Acute Care Surg, 2017; 82(4); 771-75
12. Limaiem F, Arfa N, Marsaoui L, Unexpected histopathological findings in appendectomy specimens: A retrospective study of 1627 cases: Indian J Surg, 2015; 77(Suppl 3); 1285-90
13. Murphy EM, Farquharson SM, Moran BJ, Management of an unexpected appendiceal neoplasm: Br J Surg, 2006; 93; 783-92
14. Ramaswamy V, Pathology of mucinous appendiceal tumors and pseudomyxoma peritonei: Indian J Surg Oncol, 2016; 7; 258-67
15. Inubashiri E, Watanabe Y, Akutagawa N, An incidental finding of low grade appendiceal mucinous neoplasm during cesarean section: A case report: JGH Open, 2020; 4; 306-8
16. Köhler F, Matthes N, Rosenfeldt M, Neoplasms of the appendix: Dtsch Arztebl Int, 2023; 120(31–32); 519-25
17. Panarelli NC, Yantiss RK, Mucinous neoplasms of the appendix and peritoneum: Arch Pathol Lab Med, 2011; 135; 1261-68
18. Smeenk RM, van Velthuysen MLF, Verwaal VJ, Zoetmulder FAN, Appendiceal neoplasms and pseudomyxoma peritonei: A population-based study: Eur J Surg Oncol, 2008; 34; 196-201
19. Andreopoulou E, Yee H, Warycha M, Mucinous cancer of the appendix: Challenges in diagnosis and treatment: J Chemother, 2007; 19; 451-54
20. Abdu B, Hobgood D, Stallings S, Depasquale S, Incidental finding of pseudomyxoma peritonei at primary cesarean section: Am J Perinatol, 2009; 26; 633-35
21. Erika H, Dal Y, Paul S, Management of appendiceal pseudomyxoma peritonei diagnosed during pregnancy: World J Surg Oncol, 2009; 7; 48
22. Kalu E, Croucher C, Appendiceal mucocele: A rare differential diagnosis of a cystic right adnexal mass: Arch Gynecol Obstet, 2005; 271; 86-88
23. Andersen B, Nielsen T, Appendicitis in pregnancy: Diagnosis, management and complications: Acta Obstet Gynecol Scand, 1999; 78; 758-62
24. Low RN, Barone RM, Imaging for peritoneal metastases: Surg Oncol Clin N Am, 2018; 27(3); 425-42
25. Villa M, Sforza D, Siragusa L, A low-grade appendiceal mucinous neoplasia and neuroendocrine appendiceal collision tumor: A case report and review of the literature: Am J Case Rep, 2021; 22; e927876
26. Ray JG, Vermeulen MJ, Bharatha A, Association between MRI exposure during pregnancy and fetal and childhood outcomes: JAMA, 2016; 316(9); 952-61
27. Ahmed N, Vimplis S, Deo N, A mucocele of the appendix seen as an adnexal mass on ultrasound scan: J Obstet Gynaecol, 2016; 37(1); 116-17
28. Smolkin C, Kiridly A, Pryor A, Appendicitis during pregnancy: best surgical practices and clinical management: Open Access Surg, 2023; 16; 95-103
29. Borges AL, Reis-de-Carvalho C, Chorão M, Low-grade mucinous appendiceal neoplasm mimicking an ovarian lesion: A case report and review of literature: World J Clin Cases, 2021; 9(10); 2334-43
30. Fourie H, Al Memar M, Tuomey M, The ‘onion skin’ sign of a low-grade appendiceal mucinous neoplasm: An incidental finding during early pregnancy assessment: Australas J Ultrasound Med, 2024; 27(2); 131-35
31. Pickhardt PJ, Levy AD, Rohrmann CA, Kende AI, Primary neoplasms of the appendix: Radiologic spectrum of disease with pathologic correlation: Radiographics, 2003; 23(3); 645-62
32. Van Hooser A, Williams TR, Myers DT, Mucinous appendiceal neoplasms: Pathologic classification, clinical implications, imaging spectrum and mimics: Abdom Radiol, 2018; 43; 2913-22
33. Yousef A, Yousef M, Zeineddine MA, Serum tumor markers and outcomes in patients with appendiceal adenocarcinoma: JAMA Netw Open, 2024; 7(2); e240260
34. Schmoeckel E, Kirchner T, Mayr D, SATB2 is a supportive marker for the differentiation of a primary mucinous tumor of the ovary and an ovarian metastasis of a low-grade appendiceal mucinous neoplasm (LAMN): A series of seven cases: Pathol Res Pract, 2018; 214(3); 426-30
Figures
Figure 1. (A–D) Low-grade appendiceal mucinous neoplasm (LAMN). (A–C) Proliferation of mucinous epithelial cells forming villous structures within the appendiceal lumen. The underlying lymphoid tissue is atrophic, and the muscularis mucosae is effaced. Subepithelial fibrosis is present, and the lesion demonstrates a pushing (non-infiltrative) growth pattern. (D) The lesional epithelium shows abundant apical mucin and elongated nuclei with mild (low-grade) cytologic atypia. (H&E; magnifications: A ×40; B ×100; C ×200; D ×400).Figure 2. (A, B) Extruded mucin. (A) Mucin pools covering the serosa with a prominent granulation tissue response. (B) Extruded mucin surrounded by granulation tissue composed of fibroblasts, blood vessels and inflammatory cells. (H&E; magnifications: ×100). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133