23 December 2025: Articles 
Platypnea-Orthodeoxia Syndrome Associated With a Right-to-Left Cardiac Shunt Detected by Lung Perfusion Scintigraphy
Challenging differential diagnosis, Rare disease
Yusuke NakanoDOI: 10.12659/AJCR.949642
Am J Case Rep 2025; 26:e949642






Abstract
BACKGROUND: Platypnea-orthodeoxia syndrome is a rare condition characterized by posture-dependent right-to-left shunting, resulting in dyspnea in the upright position that improves when supine. Diagnosis usually relies on echocardiographic microbubble testing or transesophageal echocardiography, which require patient cooperation and cardiology support and may be impractical in older or psychiatric patients. Lung perfusion scintigraphy provides a practical, noninvasive alternative for detecting shunts without requiring cooperation or cardiologist involvement. This report describes a case of platypnea-orthodeoxia syndrome associated with a right-to-left cardiac shunt that was detected by lung perfusion scintigraphy.
CASE REPORT: A 64-year-old woman with hypertension and severe bipolar disorder was admitted after being found unconscious. She displayed persistent hypoxemia despite oxygen supplementation. Laboratory findings were unremarkable; imaging revealed a dilated aortic root compressing the right atrium but no evidence of pulmonary embolism or pneumonia. Transthoracic echocardiography showed no definitive shunt. Microbubble testing or transesophageal echocardiography could not be performed due to psychiatric instability and lack of immediate cardiology support. On hospital day 2, lung perfusion scintigraphy demonstrated a right-to-left shunt, whereas chest computed tomography excluded intrapulmonary shunting. Cardiac catheterization on day 5 confirmed a patent foramen ovale with right atrial compression, establishing the diagnosis of platypnea-orthodeoxia syndrome. Shunt closure was deferred due to the unavailability of a specialist for percutaneous closure. At 12 months of follow-up, the patient remained untreated.
CONCLUSIONS: Lung perfusion scintigraphy represents a noninvasive and effective diagnostic tool for identifying intracardiac shunting in patients with unexplained hypoxemia when microbubble testing or transesophageal echocardiography is not feasible.
Keywords: Bipolar Disorder, Cardiac Imaging Techniques, Radionuclide Imaging, Technetium Tc 99m Aggregated Albumin, Humans, Female, Middle Aged, Dyspnea, hypoxia, Syndrome, Foramen Ovale, Patent, perfusion imaging, Posture, Lung, Platypnea Orthodeoxia Syndrome
Introduction
Platypnea-orthodeoxia syndrome (P-OS) is a rare condition characterized by posture-dependent right-to-left shunting at the atrial level, which results in dyspnea in the upright position with improvement when supine [1,2]. In intracardiac shunt disorders, including P-OS, accurate diagnosis requires definitive demonstration of a right-to-left shunt [3], typically achieved through echocardiography with microbubble contrast or transesophageal echocardiography [4]. However, these procedures require patient cooperation – such as breath-holding – and may cause discomfort, making them difficult to perform in older adults or patients with psychiatric disorders. Furthermore, the examinations and their interpretation generally require cardiologist involvement, limiting feasibility in facilities without cardiology support.
In most reported cases, the diagnosis of intracardiac shunt disorders has been triggered by echocardiography [5,6]. In contrast, lung perfusion scintigraphy offers a practical alternative for detecting and quantifying intracardiac shunts, including those associated with P-OS [7]. This technique allows rapid assessment even in patients who cannot cooperate due to psychiatric comorbidities [8,9], and it can be performed without cardiologist involvement. Despite these advantages, lung perfusion scintigraphy remains underused in clinical practice, and its diagnostic value is often underrecognized.
This report describes a 64-year-old woman who displayed P-OS associated with a right-to-left cardiac shunt caused by a patent foramen ovale, which was successfully diagnosed via lung perfusion scintigraphy.
Case Report
A 64-year-old Japanese woman was found unconscious by a passerby and transported to our hospital. Her medical history included hypertension and severe bipolar disorder, for which she was not receiving treatment. Due to her psychiatric condition, she was unable to engage in meaningful communication. There was no notable family history. On arrival, the patient was alert, with a Glasgow Coma Scale score of E4V4M6. Vital signs were as follows: body temperature, 36.6°C; blood pressure, 154/98 mmHg; heart rate, 108 beats/min (regular); and oxygen saturation, 85% while receiving 4 L/min oxygen via face mask in the semi-sitting position. Physical examination revealed no conjunctival pallor. Chest auscultation revealed no murmurs, rubs, or adventitious sounds. No neurological deficits, including paralysis, were observed. Because of persistent hypoxemia, the patient was admitted to the respiratory medicine ward for further evaluation.
Laboratory tests at admission demonstrated mild hepatic enzyme elevation and polycythemia (Table 1), whereas B-type natriuretic peptide levels were within the normal range. Arterial blood gas analysis on room air in the supine position revealed pronounced hypoxemia (PaO2 53.7 mmHg, oxygen saturation 87.0%) (Table 1). Chest radiography showed cardiomegaly and right hilar enlargement, likely secondary to dilation of the aortic root, without evidence of aneurysm, pleural effusion, or pneumonia (Figure 1A). Chest computed tomography (CT) revealed mild post-inflammatory changes in the right middle lobe but no pulmonary arteriovenous malformation. Contrast-enhanced CT showed compression of the right atrium by the dilated aorta (Figure 1B), but pulmonary embolism was absent. Electrocardiography indicated left axis deviation without other notable abnormalities. Transthoracic echocardiography revealed a dilated aortic root (Figure 2A), which obscured visualization of the right atrium, tricuspid valve, and atrial septum; there were no other clinically significant findings. These results excluded heart failure, pneumonia, and pulmonary embolism as causes of hypoxemia. However, a right-to-left shunt remained a possible explanation. Although echocardiographic microbubble testing or transesophageal echocardiography would typically be required [4], these examinations were not feasible because the patient could not follow instructions due to severe bipolar disorder, and cardiology support for transesophageal echocardiography was not immediately available.
Therefore, lung perfusion scintigraphy, which can be performed without patient cooperation or cardiology involvement, was conducted on the second hospital day. Ventilation scans excluded ventilation-perfusion mismatch suggestive of pulmonary embolism. However, substantial technetium-99m uptake was noted in the thyroid and kidneys, consistent with a right-to-left shunt (Figure 2B). Based on these findings, the respiratory medicine team referred the patient to cardiology for further evaluation. On the fifth hospital day, sedated cardiac catheterization was performed with family consent. A guidewire was advanced smoothly from the right atrium to the left atrium, confirming patent foramen ovale. Right atriography demonstrated compression of the right atrium by the dilated aorta (Figure 2C). Pulmonary vascular resistance and right-sided heart pressures were within normal limits, but a right-to-left shunt was confirmed (Table 2). Coronary angiography revealed no clinically significant coronary artery disease. Collectively, these findings established a diagnosis of P-OS caused by right-to-left shunting through a patent foramen ovale. The mechanism was attributed to anatomical alteration from right atrial compression by the dilated aorta, which facilitated posture-dependent shunting.
The definitive treatment for P-OS is shunt closure [10]. Although invasive investigations were performed with family consent, our institution did not have a specialist qualified to perform percutaneous shunt closure; therefore, closure was not undertaken during catheterization. Because of the patient’s psychiatric instability and lack of symptom awareness while supine, surgical intervention was not pursued; treatment was deferred until symptom progression clearly warranted intervention. Subsequently, the patient’s psychiatric condition deteriorated, and she became largely bedridden in the psychiatric ward. At 12 months of follow-up, shunt closure had not been performed.
Discussion
This case highlights the diagnostic value of lung perfusion scintigraphy for P-OS, a rare disorder characterized by right-to-left shunting. A 64-year-old woman with severe bipolar disorder presented with unexplained hypoxemia and posture-dependent dyspnea that required further evaluation for a right-to-left shunt. Diagnostic procedures such as echocardiographic microbubble testing or transesophageal echocardiography, which require patient cooperation and cardiology support, were not feasible. Instead, lung perfusion scintigraphy demonstrated a right-to-left shunt, and subsequent cardiac catheterization confirmed the diagnosis of P-OS.
P-OS is a rare condition in which dyspnea and hypoxemia worsen in the upright position and improve when supine [1–3]. This phenomenon is attributed to postural changes that affect interatrial shunting [2,3]. Right-to-left shunting in P-OS results from both anatomical and mechanical factors. Anatomically, a patent foramen ovale or atrial septal defect provides a channel for shunting. Mechanically, elongation or dilation of the aorta may compress the right atrium, producing septal deformation in the upright position [11,12]. In the present case, both anatomical (a patent foramen ovale) and mechanical (right atrial compression by a dilated aorta of uncertain cause) factors were present, likely contributing to P-OS development. In most previously reported cases, the intracardiac shunt was readily detected because patients could cooperate with echocardiographic testing [5,6]. Although right atrial compression was evident on chest CT, the patent foramen ovale was not visualized on transthoracic echocardiography; microbubble testing was not possible due to the patient’s psychiatric condition and lack of immediate cardiology support. Lung perfusion scintigraphy revealed a right-to-left shunt, whereas chest CT excluded intrapulmonary shunting, thus guiding subsequent invasive evaluation via cardiac catheterization.
Lung perfusion scintigraphy enables the detection and quantification of intracardiac and intrapulmonary right-to-left shunts through intravenous administration of technetium-99m-labeled macroaggregated albumin [7–9]. Particles larger than 10 μm are usually trapped within the pulmonary capillary bed. In the presence of a right-to-left shunt, however, some particles bypass the lungs and accumulate in systemic organs such as the thyroid and kidneys [7–9]. In the present case, clear uptake in these organs provided definitive evidence of systemic tracer distribution and confirmed the presence of a right-to-left shunt. This modality is rapid, minimally invasive, and does not require heavy sedation, making it particularly valuable when an intracardiac shunt is suspected but microbubble testing or transesophageal echocardiography cannot be performed. Such situations include older or uncooperative patients [9,13,14]; those with contagious respiratory infections such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); patients with a pronounced gag reflex [8,9]; and individuals with oral, pharyngeal; or esophageal abnormalities that preclude transesophageal echocardiography [8,9].
Conclusions
Lung perfusion scintigraphy represents a noninvasive and effective diagnostic tool for detecting intracardiac shunting in patients with unexplained hypoxemia when microbubble testing or transesophageal echocardiography is not feasible. This case highlights the importance of including lung perfusion scintigraphy in the diagnostic evaluation of intracardiac shunts such as P-OS and reaffirms the value of this imaging modality in complex clinical scenarios.
Figures
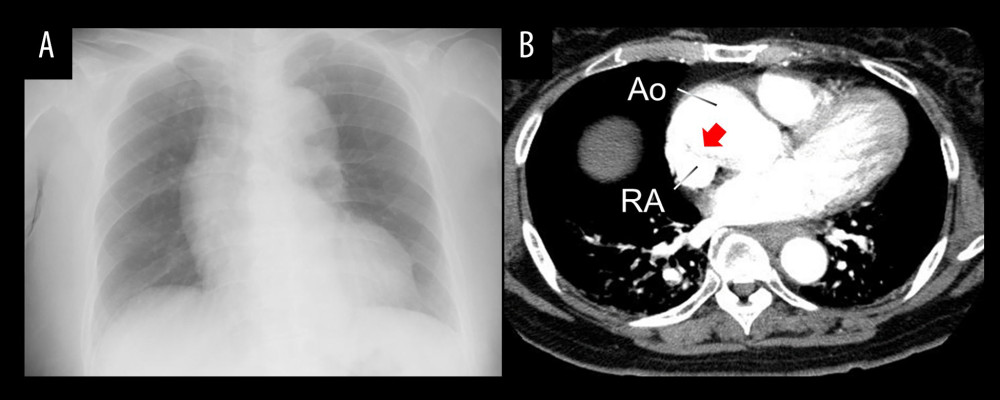 Figure 1. Chest imaging findings. (A) Chest X-ray showing mild cardiomegaly and dilation of the right pulmonary hilum. (B) Contrast-enhanced chest CT scan demonstrating compression of the right atrium by an enlarged ascending aorta (red arrow). CT – computed tomography; Ao – aorta; RA – right atrium.
Figure 1. Chest imaging findings. (A) Chest X-ray showing mild cardiomegaly and dilation of the right pulmonary hilum. (B) Contrast-enhanced chest CT scan demonstrating compression of the right atrium by an enlarged ascending aorta (red arrow). CT – computed tomography; Ao – aorta; RA – right atrium. 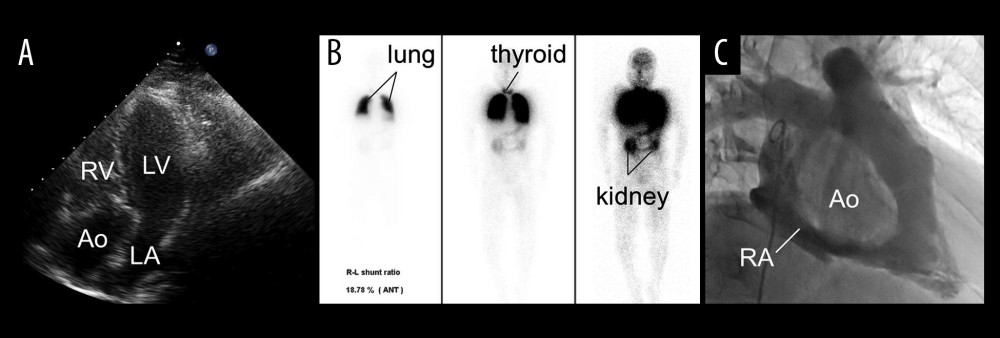 Figure 2. Cardiac and scintigraphic findings. (A) Apical 4-chamber view on transthoracic echocardiography showing an enlarged aortic root (Ao) obscuring visualization of the right atrium, tricuspid valve, and interatrial septum, where a shunt would usually be identified. (B) Lung perfusion scintigraphy demonstrating technetium-99m (99mTc) particle uptake in the thyroid (middle) and kidneys (right) in addition to the lungs (left), indicating systemic distribution due to a right-to-left shunt. (C) Right atriography showing compression of the right atrium by the dilated ascending aorta (Ao). 99mTc – technetium-99m-labeled macroaggregated albumin; Ao – aorta; RV – right ventricle; LV – left ventricle; LA – left atrium; RA – right atrium.
Figure 2. Cardiac and scintigraphic findings. (A) Apical 4-chamber view on transthoracic echocardiography showing an enlarged aortic root (Ao) obscuring visualization of the right atrium, tricuspid valve, and interatrial septum, where a shunt would usually be identified. (B) Lung perfusion scintigraphy demonstrating technetium-99m (99mTc) particle uptake in the thyroid (middle) and kidneys (right) in addition to the lungs (left), indicating systemic distribution due to a right-to-left shunt. (C) Right atriography showing compression of the right atrium by the dilated ascending aorta (Ao). 99mTc – technetium-99m-labeled macroaggregated albumin; Ao – aorta; RV – right ventricle; LV – left ventricle; LA – left atrium; RA – right atrium. References
1. Seward JB, Hayes DL, Smith HC, Platypnea-orthodeoxia: Clinical profile, diagnostic workup, management, and report of seven cases: Mayo Clin Proc, 1984; 59; 221-31
2. Knapper JT, Schultz J, Das G, Sperling LS, Cardiac platypnoea-orthodeoxia syndrome: An often unrecognized malady: Clin Cardiol, 2014; 37; 645-49
3. Lombardi M, Del Buono MG, Princi G, Platypnea-orthodeoxia syndrome as an uncommon cause of dyspnoea: A literature review: Intern Med J, 2022; 52; 921-25
4. Nagueh SF, Smiseth OA, Appleton CP, Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging: J Am Soc Echocardiogr, 2016; 29; 277-314
5. Borgaonkar SP, Lam WW, Razavi M, Parekh DR, Platypnea-orthodeoxia syndrome caused by an intracardiac shunt: Tex Heart Inst J, 2020; 47; 298-301
6. Dodson BK, Major CK, Grant M, Platypnea orthodeoxia due to a patent foramen ovale and intrapulmonary shunting after severe COVID-19 pneumonia: Am J Case Rep, 2021; 22; e933975
7. Roach PJ, Gradinscak DJ, Schembri GP, SPECT/CT in V/Q scanning: Semin Nucl Med, 2010; 40; 455-66
8. Parker JA, Coleman RE, Grady E, SNM practice guideline for lung scintigraphy 4.0: J Nucl Med Technol, 2012; 40; 57-65
9. Chokkappan K, Kannivelu A, Srinivasan S, Babut SB, Review of diagnostic uses of shunt fraction quantification with technetium-99m macroaggregated albumin perfusion scan as illustrated by a case of Osler-Weber-Rendu syndrome: Ann Thorac Med, 2016; 11; 155-60
10. Stout KK, Daniels CJ, Aboulhosn JA, 2018 AHA/ACC Guideline for the management of adults with congenital heart disease: executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: Circulation, 2019; 139; e637-e97
11. Popp G, Melek H, Garnett AR, Platypnea-orthodeoxia related to aortic elongation: Chest, 1997; 112; 1682-84
12. Al Saadi W, Al-Lawati AI, Al Busaidi M, Platypnea-orthodeoxia syndrome caused by patent foramen ovale with right-to-left shunt: Am J Case Rep, 2023; 24; e942216
13. Gates GF, Orme HW, Dore EK, Cardiac shunt assessment in children with macroaggregated albumin technetium-99m: Radiology, 1974; 112; 649-53
14. Ptaszek LM, Saldana F, Palacios IF, Wu SM, Platypnea-orthodeoxia syndrome in two previously healthy adults: A case-based review: Clin Med Cardiol, 2009; 3; 37-43
Figures
Figure 1. Chest imaging findings. (A) Chest X-ray showing mild cardiomegaly and dilation of the right pulmonary hilum. (B) Contrast-enhanced chest CT scan demonstrating compression of the right atrium by an enlarged ascending aorta (red arrow). CT – computed tomography; Ao – aorta; RA – right atrium.Figure 2. Cardiac and scintigraphic findings. (A) Apical 4-chamber view on transthoracic echocardiography showing an enlarged aortic root (Ao) obscuring visualization of the right atrium, tricuspid valve, and interatrial septum, where a shunt would usually be identified. (B) Lung perfusion scintigraphy demonstrating technetium-99m (99mTc) particle uptake in the thyroid (middle) and kidneys (right) in addition to the lungs (left), indicating systemic distribution due to a right-to-left shunt. (C) Right atriography showing compression of the right atrium by the dilated ascending aorta (Ao). 99mTc – technetium-99m-labeled macroaggregated albumin; Ao – aorta; RV – right ventricle; LV – left ventricle; LA – left atrium; RA – right atrium. Tables
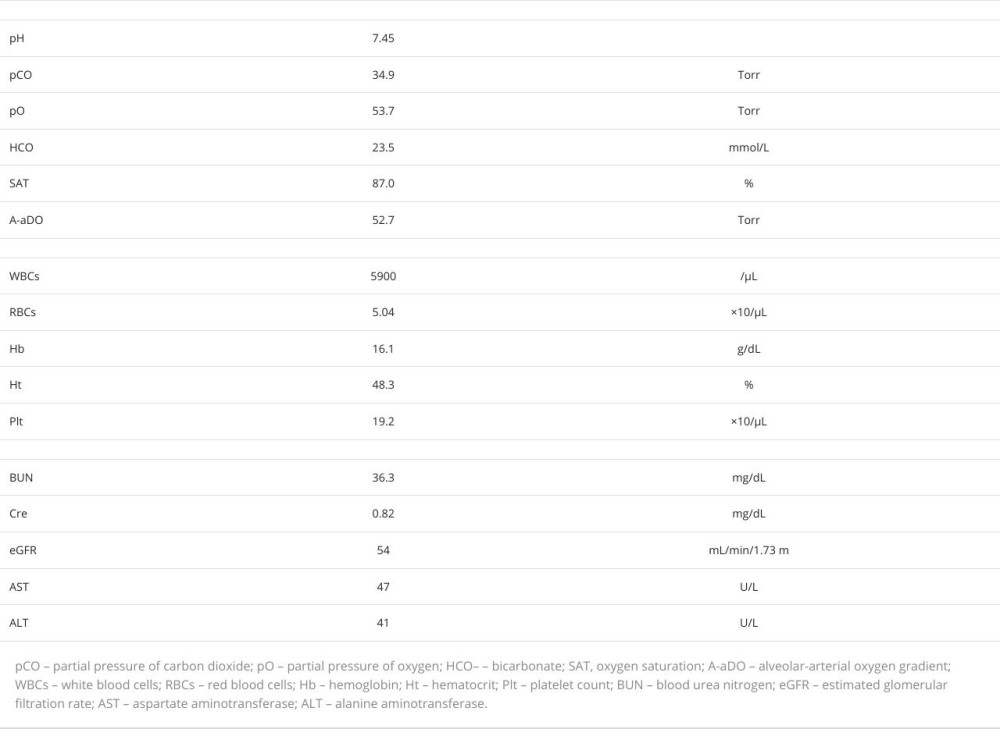 Table 1. Admission laboratory data: supine hypoxemia with mild hepatic dysfunction and polycythemia.
Table 1. Admission laboratory data: supine hypoxemia with mild hepatic dysfunction and polycythemia.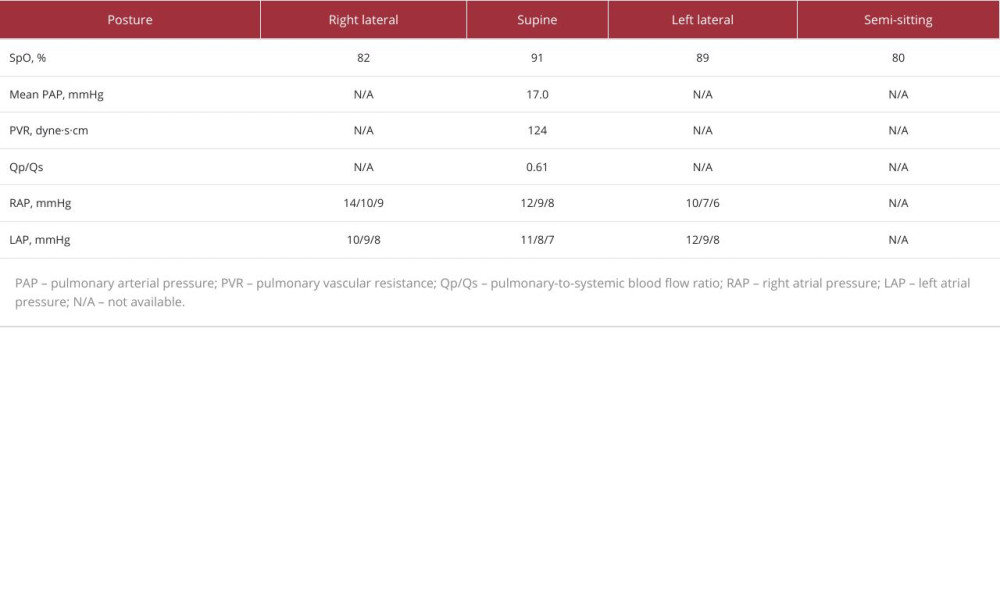 Table 2. Oxygen saturation and right and left atrial pressures in various postures.Table 1. Admission laboratory data: supine hypoxemia with mild hepatic dysfunction and polycythemia.Table 2. Oxygen saturation and right and left atrial pressures in various postures.
Table 2. Oxygen saturation and right and left atrial pressures in various postures.Table 1. Admission laboratory data: supine hypoxemia with mild hepatic dysfunction and polycythemia.Table 2. Oxygen saturation and right and left atrial pressures in various postures. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133