29 December 2025: Articles 
Rapidly Progressive Disseminated Bacillus Calmette-Guérin Infection (BCGitis) in a 3-Month-Old Infant Without Immunodeficiency: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unexpected drug reaction
Nathalya Queiroz Perillo EF 1, Taynara HeliodoroDOI: 10.12659/AJCR.949742
Am J Case Rep 2025; 26:e949742






Abstract
BACKGROUND: Disseminated Bacillus Calmette-Guérin (BCG) disease is a rare but severe complication of BCG vaccination, particularly in immunocompromised children, and is associated with high mortality. The incidence of disseminated Bacillus Calmette-Guérin disease is approximately 1.56 to 4.29 cases per million vaccinated individuals, with an overall mortality of 60% to 80%. Lesions most commonly appear in the right arm, axilla, and areas adjacent to the injection site. We report a case of a rare presentation of disseminated BCGitis 3 months after the intradermal vaccine.
CASE REPORT: A previously healthy 3-month-old infant developed devastating skin, subcutaneous, bone, lymphatic, and systemic complications located in the head and neck. The rapidly progressive and destructive growth of the lesions simulated a malignant neoplasm. After several weeks of investigation and challenging diagnosis, the patient was successfully treated with a 7-month regimen of rifampicin, isoniazid, and ethambutol, with resolution and no sequelae. No underlying immunodeficiency was identified. At 3-year follow-up, the child demonstrated normal neurodevelopment and psychomotor function, with no significant infections or other immune-related problems.
CONCLUSIONS: Disseminated BCGitis can be the first manifestation of a primary immunodeficiency or secondary immunodeficiency or can occur sporadically, as in our patient. The condition can progress rapidly and be fatal, making early recognition essential.
Keywords: BCG Vaccine, Immune System, Isoniazid, Mycobacterium, Temporal Bone, Humans, Infant, Antitubercular Agents, Mycobacterium bovis, Tuberculosis
Introduction
The tuberculosis (TB) vaccine, Bacillus Calmette-Guérin (BCG), is a live attenuated bacilli of
The presentation forms of BCGitis can be recognized in its natural evolution. Non-suppurative BCGitis occurs earlier and usually resolves spontaneously within a few weeks without any sequelae. In some cases, the affected ganglion progressively increases in size and develops suppuration, swelling, and erythema of the underlying skin. Suppurative BCGitis can develop after 2 to 4 months of BCG vaccination and persist for several months. BCGitis occurrence is most commonly secondary to immune deficiency, especially primary immunodeficiency [6,7]. We report a case of a previously healthy patient without detected immune system deficiencies before the diagnosis. In our literature search, we did not find any reported cases of disseminated BCGitis affecting the ear, temporal bone, or parotid gland or simulating a neoplasm in the head and neck.
Case Report
A previously healthy 3-month-old male infant presented with a daily purulent otorrhea unilaterally in the right ear for 1 month, which was refractory to oral antibiotic therapy. This was associated with high fever, irritability, prostration, and weight loss. Even with the administration of broad-spectrum antibiotics, after 1 week of hospitalization, the patient developed progressive growth of an infra-auricular and right retroauricular cervical mass. The mass continued to enlarge and, 2 weeks later, measured approximately 2.5×2.0 cm with phlogosis and a drainage point, in addition to ipsilateral suppurative lymphadenitis. There was associated ipsilateral axillary lymphadenopathy. In the third week, the lesion evolved with an ulcerative-vegetative appearance (Figure 1). Ultrasound examination revealed lymph node enlargement and a lymph node conglomerate at right level II with loss of hilar morphology, measuring 2.6×1.5 cm in its largest axial dimensions. Lymph nodes increased in number, with some enlarged and showing loss of fatty hila at right level IB and bilateral levels II, III, and V, with right-sided predominance. A heterogeneous solid nodule with irregular edges was present in the right retroauricular region, associated with apparent bone erosion of the adjacent mastoid, measuring approximately 2.2×2.1 cm. The right parotid gland was enlarged with heterogeneous echotexture and intraglandular lymph node enlargement (Figure 2). Computed tomography (CT) showed an expansive lesion of the degenerative granulomatous type, with bone involvement, including the tympanic tegmen, and lymph node enlargement (Figure 3). Nuclear magnetic resonance imaging (MRI) showed an expansive and infiltrative lesion in the right cervical region. There was no involvement of the central nervous system (Figure 4).
The patient was hospitalized, and a treatment regimen with large spectrum intravenous antibiotics and corticosteroid was initiated. However, the patient still had fever, abundant purulent secretion, increasing leukocytosis, and elevated inflammatory test results for more than 4 weeks. There were no relevant occurrences of neonatal or family history, except for the maternal report of syphilis treated during the pregnancy of the patient’s 6-year-older brother. There was no parental consanguinity. The patient received BCG and hepatitis B vaccinations at birth. Serology results for HIV,
Despite all possible clinical measures and negative laboratory results, the patient’s condition continued to worsen, and we took him to the surgical center in the third week. The incisional biopsy of the lesion showed histiocytosis cells and multiple necrotizing granulomas (Figure 5), with the presence of Fite-Faraco-positive bacilliform structures, identifiable with acid-fast bacilli (Figure 6).
During the 3-year follow-up, the child presented normal neurodevelopment and psychomotor function and no other relevant infections or problems with the immune system. We do not find any immunosuppression or comorbidities. The 2 older brothers received the BCG vaccine at birth with no adverse reactions The affected area is well healed eleven months after treatment (Figure 8).
Discussion
The BCG vaccine is derived from
The most common clinical presentation is intermittent fever, unintentional weight loss, systemic or multiorgan abnormalities, and a personal previous history of any immunodeficiency. This is also described as a rare occurrence of disseminated intravascular coagulation [14]. The earliest clinical signs include local erythema that evolves to a progressive edema in the ipsilateral axillary right region (the injection site). This can develop as purulent drainage, generalized lymphadenopathy, mucocutaneous rash, bone involvement, hepatosplenomegaly, and cough. The diagnosis criteria are the existence of systemic symptoms, such as fever, fatigue, weight loss, and malaise, and 2 or more involved areas. The definitive diagnostic criteria are the presence of a BCG vaccination scar with isolation of
An important differential diagnosis is scrofuloderma due to
Primary immunodeficiency diseases are inherited disorders of the immune system that increase the susceptibility to vaccination complications and infections. The most common type of immunodeficiency disorder is severe combined immunodeficiency syndrome, followed by unspecified immunodeficiency (nonspecific changes in CD3, CD4, and CD8 counts on peripheral blood flow cytometry) [17,18]. Basic immune screening to determine underlying immune defects should include serum immunoglobulin levels (IgG, IgA, IgM, and IgE), lymphocyte subsets (CD3+, CD4+, CD8+ T cells; B cells, CD19+; and CD56+ natural killer cells), HIV serology, and neutrophil and interferon-gamma/interleukin-12 oxidation tests. In the present case, the results of these initial complementary tests were normal [19].
In addition, genetic analysis can help detect susceptibility to BCG disorders. The most commonly identified gene alleles in primary immunodeficiency diseases are
There is no consensus treatment strategy for disseminated BCGitis, either for medications or duration of treatment. Nevertheless, most reports, case series, and literature reviews report choosing to use the RIE regimen for 6 months. The regimen can be used alone or in combination with corticosteroids, and the infection usually resolves with no sequelae. The sensitivity to isoniazid and rifampicin are satisfied in general BCG vaccine strains currently in use [1–3,21]. This double combination is usually effective and non-inferior, compared with other multidrug regimens containing more than 2 antitubercular drugs. The duration of therapy can vary from months to years, depending on the response and underlying immune defects.
Moxifloxacin might be considered for about 10 months in children with BCGitis [25]. There are many reported cases with intravenous antibiotics, antivirals, and antifungals associated with antitubercular treatment, especially when the diagnosis was not fulfilled or was delayed [26,27]. Our patient was treated for 7 months with RIE, and we stopped only after complete resolution. We considered that the possible adverse effects of ethambutol (mainly impaired vision) were outweighed by the severity of this case. Isoniazid is metabolized in the liver, leading to hepatotoxic metabolites of hydrazine and acetyl hydrazine, with an incidence of 0.6% of hepatotoxicity, hepatocellular necrosis, and steatosis. Rifampicin can cause cholestasis, elevation of conjugated bilirubin, and transient transaminitis, which is often benign. Rarely, it is associated with centrilobular parenchymal necrosis [28,29].
A replacement dose of intravenous immunoglobulin is also important when specific immunosuppression is detected. Alternative vaccinations can be considered when immunosuppressants are previously known or in siblings of patients who had disseminated BCGitis, and include antigen-based vaccines,
Conclusions
We report an unusually severe course of
Figures
 Figure 1. The progressive growth of infra-auricular and right retroauricular cervical mass. The mass measures approximately 2.5×2.0 cm, with phlogosis and drainage point, in addition to ipsilateral suppurative lymphadenitis.
Figure 1. The progressive growth of infra-auricular and right retroauricular cervical mass. The mass measures approximately 2.5×2.0 cm, with phlogosis and drainage point, in addition to ipsilateral suppurative lymphadenitis. 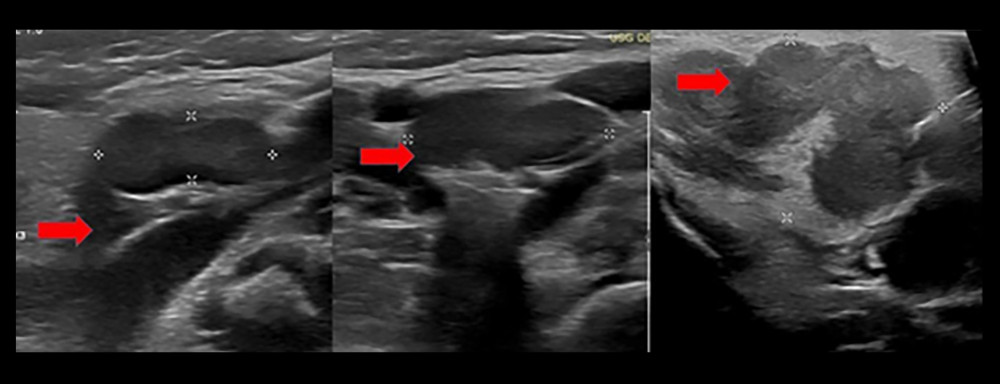 Figure 2. Ultrasound examination showing lymph node enlargement and a lymph node conglomerate at right level II, with loss of hilar architecture, measuring 2.6×1.5 cm in its largest axial dimensions. Additional lymph nodes are increased in number, with some enlarged and loss of fatty hila at right level IB and bilateral levels II, III, and V, predominating on the right.
Figure 2. Ultrasound examination showing lymph node enlargement and a lymph node conglomerate at right level II, with loss of hilar architecture, measuring 2.6×1.5 cm in its largest axial dimensions. Additional lymph nodes are increased in number, with some enlarged and loss of fatty hila at right level IB and bilateral levels II, III, and V, predominating on the right. 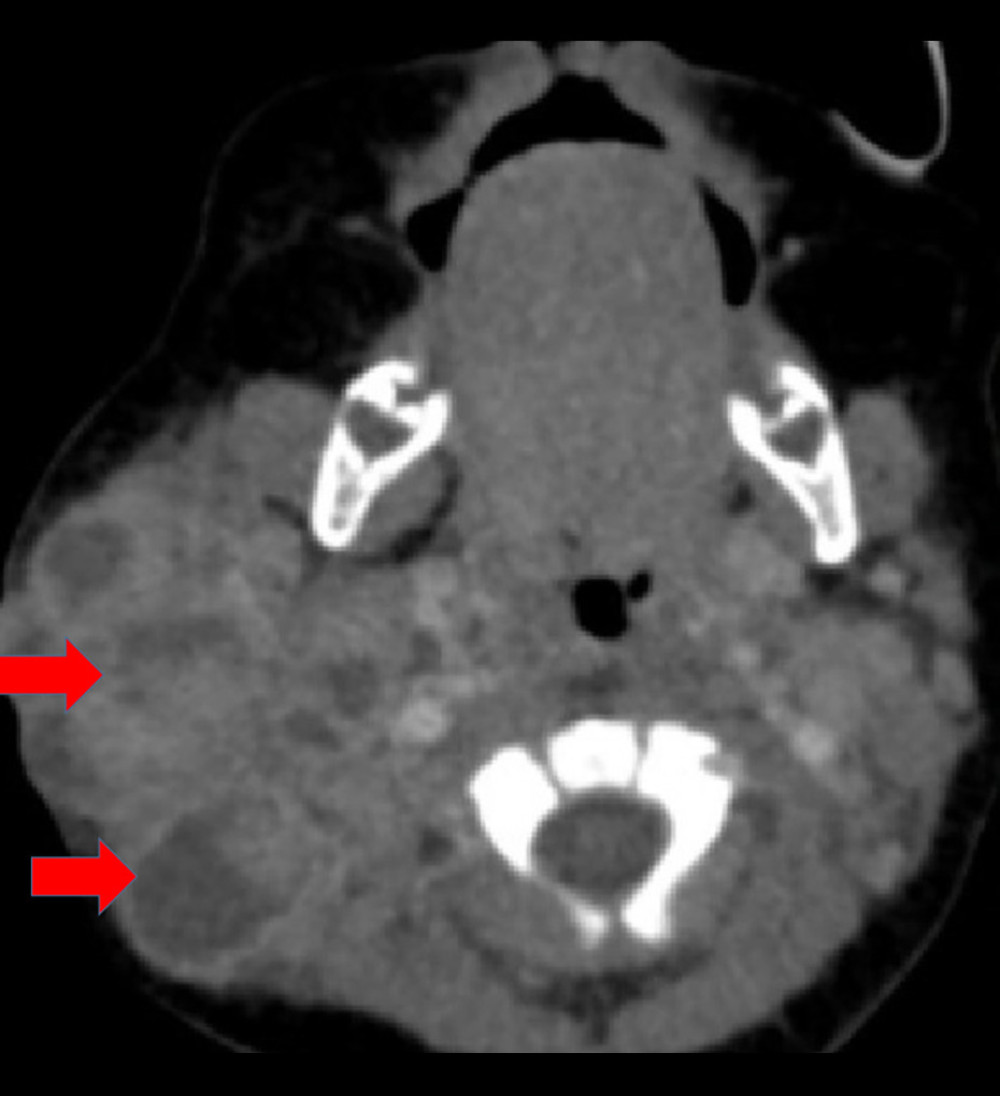 Figure 3. Computed tomography axial scan showing an expansile granulomatous lesion with bone involvement, including the tympanic tegmen, and associated lymph node enlargement.
Figure 3. Computed tomography axial scan showing an expansile granulomatous lesion with bone involvement, including the tympanic tegmen, and associated lymph node enlargement. 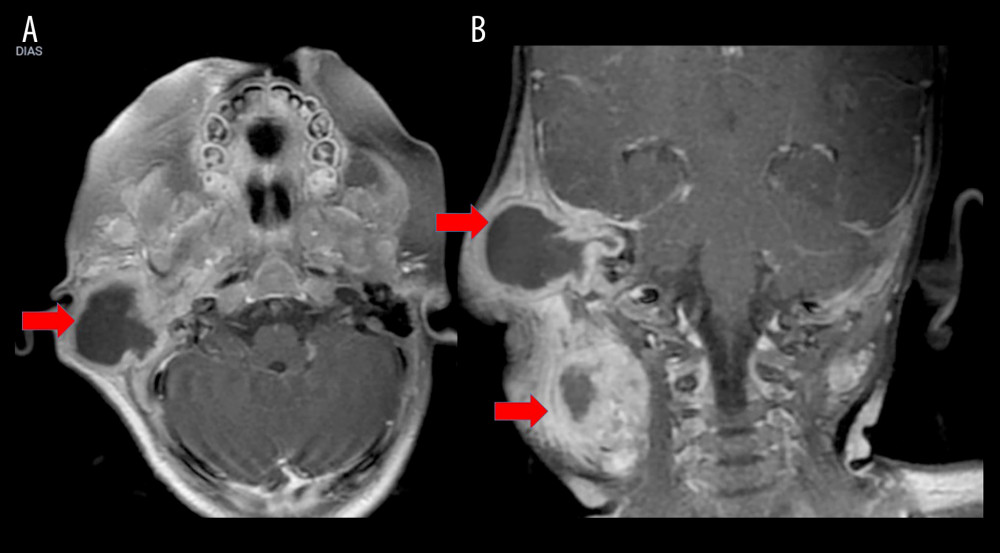 Figure 4. Nuclear magnetic resonance imaging showing an expansive and infiltrative lesion in the right cervical region. There is no involvement of the central nervous system: (A) axial section; (B) coronal section.
Figure 4. Nuclear magnetic resonance imaging showing an expansive and infiltrative lesion in the right cervical region. There is no involvement of the central nervous system: (A) axial section; (B) coronal section. 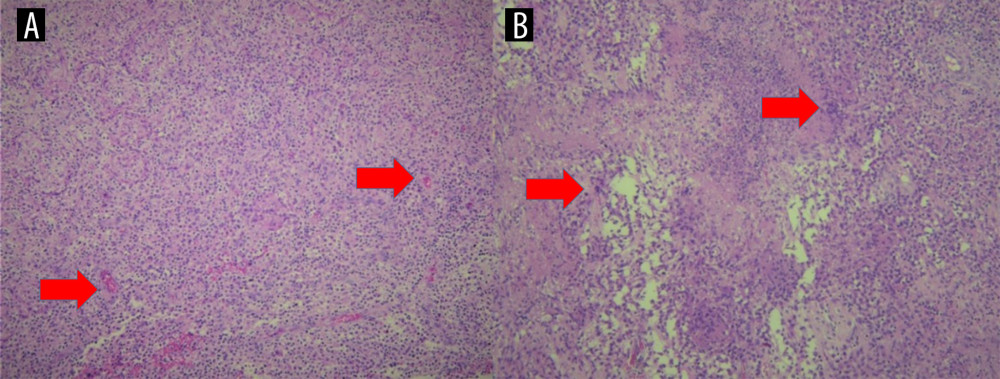 Figure 5. Anatomopathologic examination demonstrates an expansive and infiltrative lesion in the right cervical region. Hematoxylin-eosin-stained sections show histiocytic cells and multiple necrotizing granulomas. (A) Low-power magnification, ×10. (B) Higher-power magnification, ×20.
Figure 5. Anatomopathologic examination demonstrates an expansive and infiltrative lesion in the right cervical region. Hematoxylin-eosin-stained sections show histiocytic cells and multiple necrotizing granulomas. (A) Low-power magnification, ×10. (B) Higher-power magnification, ×20. 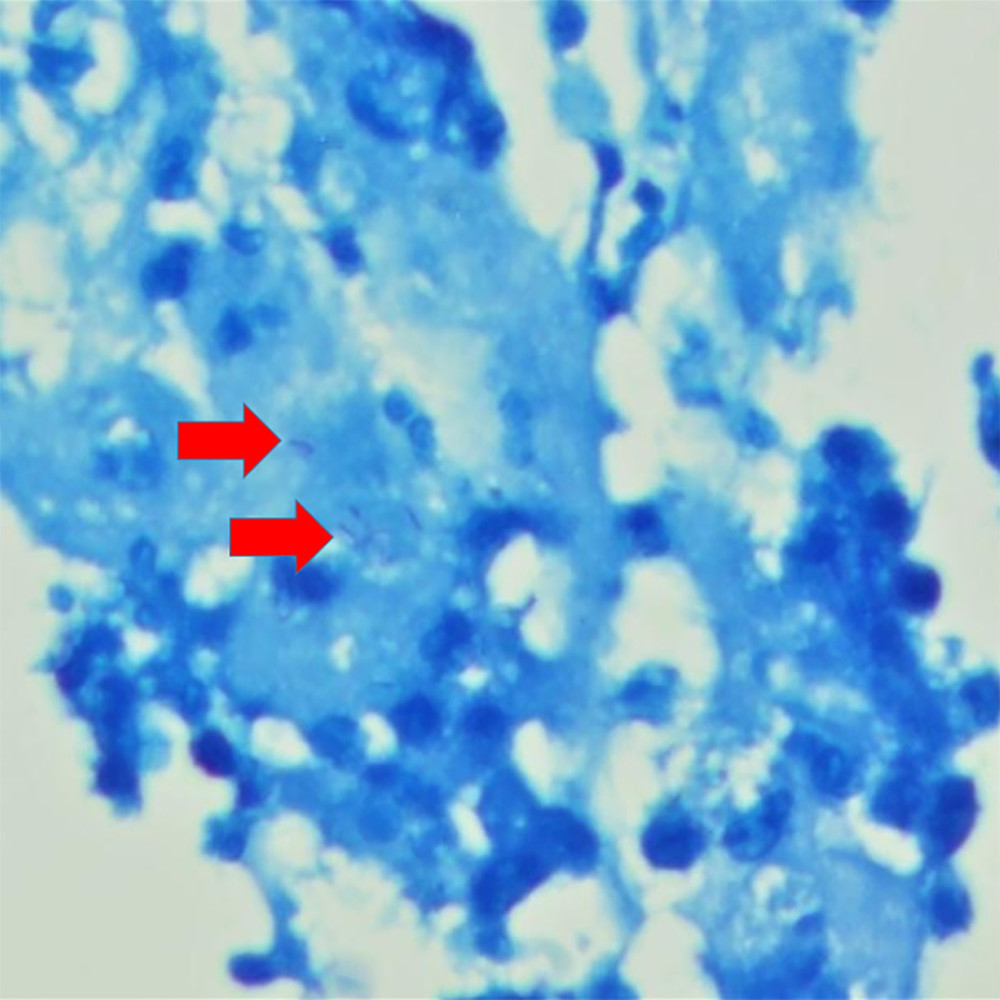 Figure 6. Fite-Faraco staining demonstrating acid-fast bacilli, ×100 magnification.
Figure 6. Fite-Faraco staining demonstrating acid-fast bacilli, ×100 magnification. 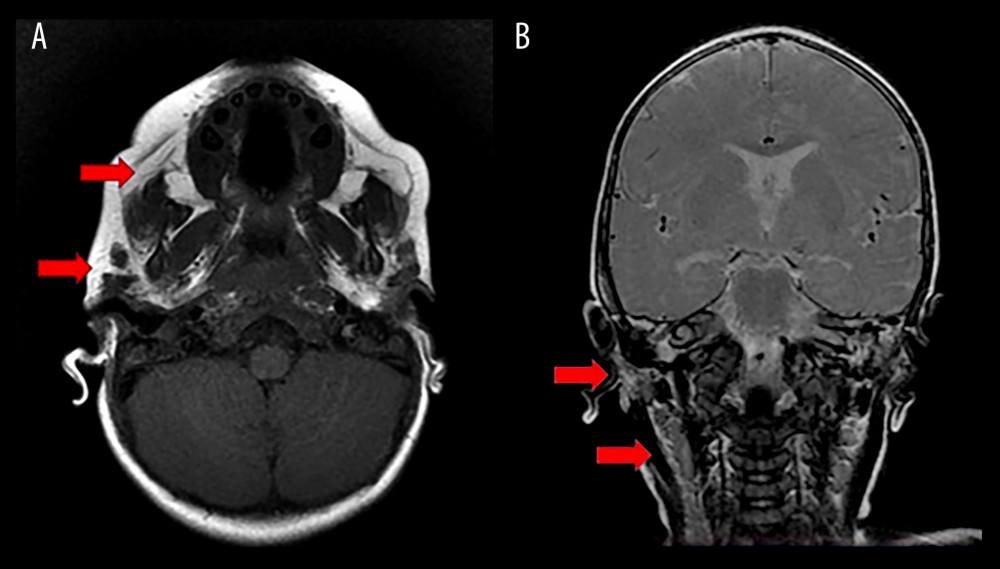 Figure 7. Nuclear magnetic resonance imaging 11 months after treatment with rifampicin, isoniazid, and ethambutol (RIE), showing complete resolution of all lesions and lymph node enlargement. (A) Axial section; (B) coronal section.
Figure 7. Nuclear magnetic resonance imaging 11 months after treatment with rifampicin, isoniazid, and ethambutol (RIE), showing complete resolution of all lesions and lymph node enlargement. (A) Axial section; (B) coronal section.  Figure 8. Appearance of the cervical lesion and right ear at last follow-up.
Figure 8. Appearance of the cervical lesion and right ear at last follow-up. References
1. Lyra PT, Souza E, Moura ACA, Inborn errors of immunity in patients with adverse events following BCG vaccination in Brazil: J Clin Immunol, 2022; 42(8); 1708-20
2. Soyak Aytekin E, Keskin A, Tan C, Differential diagnosis of primary immunodeficiency in patients with BCGitis and BCGosis: A single-centre study: Scand J Immunol, 2021; 94(4); e13084
3. Fekrvand S, Yazdani R, Olbrich P, Primary immunodeficiency diseases and Bacillus Calmette-Guérin (BCG)-vaccine-derived complications: A systematic review: J Allergy Clin Immunol Pract, 2020; 8(4); 1371-86
4. Sellami K, Amouri M, Kmiha S, Adverse reactions due to the Bacillus Calmette-Guerin vaccine: Twenty Tunisian cases: Indian J Dermatol, 2018; 63(1); 62-65
5. NaserEddin A, Dinur-Schejter Y, Shadur B, Bacillus Calmette-Guerin (BCG) vaccine-associated complications in immunodeficient patients following stem cell transplantation: J Clin Immunol, 2021; 41(1); 147-62
6. Schembri Higgans J, Pace K, Systemic BCGosis following intra-renal instillation of BCG: A case report: J Surg Case Rep, 2021; 2021(12); rjab544
7. Hesseling AC, Rabie H, Marais BJ, Bacille Calmette-Guérin vaccine-induced disease in HIV-infected and HIV-uninfected children: Clin Infect Dis, 2006; 42(4); 548-58
8. Vallilas C, Zachou M, Dolkiras P, Difficulties in diagnosing and treating disseminated Bacillus Calmette-Guérin (BCG) infection After intravesical BCG therapy in a patient with liver cirrhosis: A case report: Am J Case Rep, 2021; 22; e933006
9. Liu G, Xiao H, Liu L, Severe cases of BCGosis-susceptible primary immunodeficiency diseases identified by next-generation sequencing: Implications for adjustment of BCG vaccination timing in China: J Genet Genomics, 2020; 47(4); 229-32
10. Andrade de Souza R, Rodrigues Barreto F, Antônio de Souza Teles Santos C, Evolution of the Bacillus Calmette-Guérin scar Russia and Moreau strains in newborns: A Brazilian cohort: Vaccine X, 2023; 14; 100323
11. Diniz LM, Guimarães T, Rodrigues de Oliveira MdG: J Bras Pneumol, 2014; 40(2); 188-92
12. Sohani M, Habibi S, Delavari S, Evaluation of patients with primary immunodeficiency associated with Bacille Calmette-Guerin (BCG)-vaccine-derived complications: Allergol Immunopathol (Madr), 2020; 48(6); 729-37
13. Ladeira I, Carvalho I, Correia A, BCGitis in children: Rev Port Pneumol, 2014; 20(3); 172-73 [Erratum in: Rev Port Pneumol (2006). 2016;22(6):e1]
14. Bukhari E, Alaklobi F, Bakheet H, Disseminated bacille Calmette-Guérin disease in Saudi children: Clinical profile, microbiology, immunology evaluation and outcome: Eur Rev Med Pharmacol Sci, 2016; 20(17); 3696-702
15. Amanati A, Pouladfar G, Kadivar MR, A 25-year surveillance of disseminated Bacillus Calmette-Guérin disease treatment in children in Southern Iran: Medicine (Baltimore), 2017; 96(52); e9035
16. Barkai G, Somech R, Stauber T, Bacille Calmette-Guerin (BCG) complications in children with severe combined immunodeficiency (SCID): Infect Dis (Lond), 2019; 51(8); 585-92
17. Estrada VB, Lemos ACL, Luz PM, Scrofuloderma of the chest with mediastinal TB: Pediatr Dermatol, 2024; 41(5); 874-77
18. Hassanzad M, Valinejadi A, Darougar S, Disseminated Bacille Calmette-Guérin infection at a glance: A mini review of the literature: Adv Respir Med, 2019; 87(4); 239-42
19. Ong RYL, Chan SB, Chew SJ, Disseminated Bacillus-Calmette-Guérin infections and primary immunodeficiency disorders in singapore: A single center 15-year retrospective review: Int J Infect Dis, 2020; 97; 117-25
20. Ozsezen B, Yalçýn E, Ademhan Tural D, Antimycobacterial prophylaxis regarding Bacillus Calmette-Guérin-associated complications in children with primary immunodeficiency: Respir Med, 2022; 200; 106919
21. Elsidig N, Alshahrani D, Alshehri M, Bacillus Calmette-Guérin vaccine related lymphadenitis in children: Management guidelines endorsed by the Saudi Pediatric Infectious Diseases Society (SPIDS): Int J Pediatr Adolesc Med, 2015; 2(2); 89-95
22. Abdalla A, Elbakri AS, Almatrooshi CA, Unexpected deltoid abscess from BCG Vaccination in a healthy adult: A case report: Am J Case Rep, 2025; 26; e946723
23. Böhm WU, Koch R, Wenzel SDevelopment and treatment of localized/systemic BCGitis: Retrospective studies in direct comparison to mitomycin C: Urologe A, 2018; 57(5); 568-76 [in German]
24. Cabas P, Rizzo M, Giuffrè M, BCG infection (BCGitis) following intravesical instillation for bladder cancer and time interval between treatment and presentation: A systematic review: Urol Oncol, 2021; 39(2); 85-92
25. Alsuhaibani M, Felimban G, Shoukri M, Safety and tolerability of moxifloxacin for the treatment of disseminated BCGitis in children: Int J Pediatr Adolesc Med, 2019; 6(2); 47-50
26. Keijsers RR, Bovenschen HJ, Seyger MM, Cutaneous complication after BCG vaccination: Case report and review of the literature: J Dermatolog Treat, 2011; 22(6); 315-18
27. Lupon E, Martin-Blondel G, Pollon T, BCGitis of the wrist after intravesical BCG therapy: A case report: Hand Surg Rehabil, 2020; 39(6); 585-87
28. Roduit A, Pouget R, Defabiani N, Troillet NBCGitis following intravesical administration of bacillus Calmette-Guérin: Rev Med Suisse, 2020; 16(710); 1920-23 [in French]
29. Rajabi A, Pouladfar G, Dehghan Y, Disseminated Bacillus Calmette-Guérin infection: Role of imaging in the evaluation of complications: J Trop Pediatr, 2023; 69(4); fmad024
30. Sharma S, Tanigasalam V, Parameswaran N, Fulminant BCG disease in a 7 month old healthy male infant: J Trop Pediatr, 2015; 61(6); 474-77
31. Chitamanni P, Anbazhagan J, Parameswaran N, Vijayakumar S, BCGosis in infants with Severe Combined ImmunoDeficiency (SCID): Indian J Pediatr, 2018; 85(7); 585-86
Figures
Figure 1. The progressive growth of infra-auricular and right retroauricular cervical mass. The mass measures approximately 2.5×2.0 cm, with phlogosis and drainage point, in addition to ipsilateral suppurative lymphadenitis.Figure 2. Ultrasound examination showing lymph node enlargement and a lymph node conglomerate at right level II, with loss of hilar architecture, measuring 2.6×1.5 cm in its largest axial dimensions. Additional lymph nodes are increased in number, with some enlarged and loss of fatty hila at right level IB and bilateral levels II, III, and V, predominating on the right.Figure 3. Computed tomography axial scan showing an expansile granulomatous lesion with bone involvement, including the tympanic tegmen, and associated lymph node enlargement.Figure 4. Nuclear magnetic resonance imaging showing an expansive and infiltrative lesion in the right cervical region. There is no involvement of the central nervous system: (A) axial section; (B) coronal section.Figure 5. Anatomopathologic examination demonstrates an expansive and infiltrative lesion in the right cervical region. Hematoxylin-eosin-stained sections show histiocytic cells and multiple necrotizing granulomas. (A) Low-power magnification, ×10. (B) Higher-power magnification, ×20.Figure 6. Fite-Faraco staining demonstrating acid-fast bacilli, ×100 magnification.Figure 7. Nuclear magnetic resonance imaging 11 months after treatment with rifampicin, isoniazid, and ethambutol (RIE), showing complete resolution of all lesions and lymph node enlargement. (A) Axial section; (B) coronal section.Figure 8. Appearance of the cervical lesion and right ear at last follow-up. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133