26 December 2025: Articles 
Isolated Neck Pain as an Atypical Manifestation of Type A Acute Aortic Dissection: A Case Report
Unusual clinical course
Łukasz TurekDOI: 10.12659/AJCR.949758
Am J Case Rep 2025; 26:e949758






Abstract
BACKGROUND: Acute aortic dissection (AAD) is a life-threatening cardiovascular emergency that is most commonly associated with severe chest or back pain. Atypical symptoms such as isolated neck pain may lead to delayed diagnosis and treatment, increasing the risk of mortality. In this report, we present a diagnostically challenging case of AAD with atypical symptoms in order to increase clinical awareness and support earlier recognition of such presentations.
CASE REPORT: A 30-year-old man with obesity, a 10-pack-year smoking history, arterial hypertension, and a family history of AAD presented with isolated neck pain and a transient presyncopal episode following mild exertion. Laboratory tests showed leukocytosis and elevated D-dimer, troponin, and NT-proBNP levels. Transthoracic echocardiography raised suspicion of Type A AAD, although the initial contrast-enhanced computed tomography (CT) scan did not confirm the diagnosis. Due to continued clinical concerns, CT scan was repeated, and it revealed a Stanford Type A dissection. The patient underwent emergency surgery involving the resection of the affected segment of the ascending aorta and graft replacement using a synthetic prosthesis. His postoperative course was uneventful, and he remained asymptomatic at follow-up.
CONCLUSIONS: This case report highlights isolated neck pain as an atypical but potentially critical presentation of Type A AAD. Early recognition of atypical features in high-risk patients is essential. Multimodal imaging is crucial for timely diagnosis and improved survival outcomes.
Keywords: Case Reports, Dissection, Ascending Aorta, Early Diagnosis, Echocardiography, Neck Pain, Risk Factors
Introduction
Acute aortic dissection (AAD) is a critical and potentially fatal medical emergency that demands immediate recognition and intervention. The condition most often manifests as sudden-onset, severe pain. Contrary to older descriptions, this pain is not always ‘tearing’ or ‘ripping’, nor confined to the chest, back, or abdomen. As emphasized by the global THINK AORTA campaign [1], the pain can be transient and migratory and may mimic other conditions, which increases the risk of misdiagnosis [2,3]. As highlighted in the 2024 European Association for Cardio-Thoracic Surgery (EACTS)/Society of Thoracic Surgeons (STS) guidelines, a subset of patients with AAD may present with atypical symptoms or even no pain, which can contribute to delayed diagnosis and worse outcomes [4]. However, many patients have an unremarkable history, which increases the risk of misdiagnosis, reported in approximately 33.8% of cases [5]. Atypical presentations or symptoms result in overlap with other conditions such as acute coronary syndrome, stroke, and pulmonary embolism, often contributing to diagnostic errors. Misleading signs such as electrocardiography (ECG) changes, elevated troponin levels, and anterior chest pain may mimic other diseases. The absence of classical features such as a widened mediastinum on chest X-rays or the presence of comorbidities such as congestive heart failure can further obscure the diagnosis. Accurate recognition is improved by thorough history-taking and early use of imaging [5]. Physicians should remain alert to the possibility of aortic dissection in patients who present with symptoms such as chest pain, back pain, or syncope.
The estimated prevalence of AAD is 2.6–3.5 cases per 100 000 person-years, with a higher prevalence in men (approximately 65%) [6]. The risk increases with age, with the highest rate of occurrence in the seventh decade of life (around 63 years) [2,6]. The development of AAD is influenced by multiple factors such as arterial hypertension, preexisting aortic abnormalities, aortic valve pathology (eg, bicuspid aortic valve), previous cardiac or aortic surgery, direct blunt chest trauma, substance abuse (cocaine and amphetamines), cigarette smoking, a familial predisposition to aortic abnormalities, and advanced age [2]. These risk factors often coexist and amplify one another [2,6].
The Stanford classification system is widely used to classify AADs [7,8], distinguishing them by the presence or absence of ascending aorta involvement. Type A dissections involve the ascending aorta and typically require urgent surgical intervention. In contrast, Type B dissections are confined to the descending thoracic aorta and are often managed with medical or endovascular therapy.
In addition to these classical forms, recent imaging advancements have identified a third subtype known as non-A non-B dissections. These involve the aortic arch without affecting the ascending aorta and are characterized by an entry tear typically located between the brachiocephalic and left subclavian arteries [4]. Clinically and anatomically distinct, non-A non-B dissections may require individualized management strategies that differ from standard Type A or Type B approaches [3,4].
The most common symptom is sudden, intense pain in the back, chest, or abdomen [2,3]. Chest pain occurs in 80% of cases; back and abdominal pain is reported in 40% and 25% of cases, respectively [2]. The pain location correlates with the dissection type; anterior chest pain is more common in Type A AAD, whereas Type B AAD manifests more frequently with back or abdominal pain [2]. The pain is typically described as sharp, tearing, or ripping, with abrupt onset being the most characteristic feature [2,3]. However, approximately 6.4% of individuals do not experience any pain [6].
Another significant initial symptom of AAD is syncope, occurring in about 15% of individuals with Type A dissection and in less than 5% of those with Type B dissection [2]. It is often related to cardiac tamponade or carotid artery involvement [2,3].
Depending on the extent of aortic involvement, patients may present with additional signs and symptoms. Notable features of Type A AAD include pericardial effusion with or without cardiac tamponade, acute aortic regurgitation leading to heart failure or shock, and coronary artery involvement causing myocardial infarction [2,9]. Shock or hypotension in the setting of aortic dissection may result from several mechanisms, including rupture of the aortic wall, impaired coronary perfusion leading to myocardial infarction, acute regurgitation of the aortic valve, or accumulation of pericardial fluid causing tamponade [3,9]. Dissection may propagate to side branches, leading to end-organ ischemia or infarction, which can be fatal [2,3,6].
We present this case to highlight a diagnostically challenging and uncommon presentation of Stanford Type A AAD in a young adult, manifested solely as isolated neck pain with transient presyncope without the typical chest or back pain. This atypical symptomatology is under-reported in the literature and may easily lead to misdiagnosis or delayed treatment, both of which significantly increase mortality.
Despite the presence of well-established risk factors, including arterial hypertension, a positive family history, and smoking, the patient’s non-classical presentation could have resulted in diagnostic oversight. This case underscores the need for heightened clinical suspicion of AAD, even in younger patients presenting without classical features.
By contributing to the limited evidence on isolated neck pain as an initial manifestation of Type A dissection, this report emphasizes the importance of prompt multimodal imaging. It expands our understanding of atypical AAD presentations. It serves as a clinical reminder to include AAD in the differential diagnosis of unexplained neck pain, especially in high-risk individuals. It supports earlier recognition, reduces diagnostic delay, and improves patient outcomes.
Case Report
A 30-year-old Caucasian man with a family history of aortic dissection, a 10-pack-per-year smoking history, and obesity (body mass index: 42.6 kg/m2), with no history of other chronic diseases or disorders, was admitted to our hospital with markedly elevated blood pressure (BP), unexplained presyncope, and neck pain. His mother had a history of an AAD requiring immediate surgical intervention and survived in good condition; however, she did not undergo any genetic testing to assess for a heritable cause, and no additional familial risk factors were identified at admission.
On the day of admission, the patient performed 4 sets of squats. Soon after, he felt a sudden, brief loss of strength (presyncope) without losing consciousness, along with neck pain that lasted about 2 minutes. Previously, physical exertion had not caused any discomfort. On the day of the incident, his maximum recorded BP was 234/130 mmHg. He had no prior history of BP monitoring. Three weeks earlier, he had experienced a respiratory infection characterized by fever, cough, and a runny nose, which resolved without the need for antibiotic treatment.
Upon admission, the patient was asymptomatic. Physical examination revealed elevated BP (140/100 mmHg) without differences between the upper limbs. No other abnormalities were found, including symmetric peripheral pulses. Laboratory tests revealed leukocytosis (14.36×109/L; normal: 4.23–9.07×109/L) and elevated D-dimer (1039 μg/L; normal: 0–500 μg/L), C-reactive protein (7.52 mg/L; normal: 0.6–5 mg/L), high-sensitive cardiac troponin T (74.4–80.1 ng/L; normal: 0–14.1 ng/L), and NT-proBNP (1599 pg/mL; normal: 0–125 pg/mL). Other parameters, including kidney and liver function test results, platelet and red blood cell counts, thyroid hormone levels, lipid panel results, and HbA1c, were within normal ranges.
A 12-lead ECG revealed a normal sinus rhythm and voltage criteria consistent with left ventricular (LV) hypertrophy. Head computed tomography (CT) demonstrated no abnormalities.
In the context of elevated cardiac biomarkers – NT-proBNP and high-sensitivity troponin T – suggesting cardiac abnormalities, transthoracic echocardiography (TTE) was performed to assess for potential cardiac dysfunction or wall motion abnormalities. Although chest pain was absent, the presence of transient presyncope and hypertension prompted further evaluation for less common causes of hemodynamic stress. Unexpectedly, TTE revealed signs consistent with Type A aortic dissection, including the presence of a double lumen separated by an intimal flap. TTE also suggested LV concentric hypertrophy (LV mass index: 311.86 g/m2, relative wall thickness: 0.98, end-diastolic inferolateral wall thickness: 26 mm, end-diastolic interventricular septal wall thickness: 24 mm) (Figure 1). Resting LV outflow tract obstruction was not observed, and provocative maneuvers to assess the LV outflow tract gradient were not performed. The LV ejection fraction was normal, with mild aortic valve regurgitation and a moderate pericardial effusion (Figures 1, 2) without signs of tamponade. Two-dimensional imaging revealed dilation of the aortic root, ascending aorta and aortic arch (aortic dimensions: sinus of Valsalva, 43 mm; ascending aorta, 43 mm; mid-aortic arch, 37 mm), and the appearance of 2 vascular lumina (true and false) separated by an intimal flap, indicative of ascending aortic dissection extending into the proximal aortic arch (Figures 3, 4).
Given the echocardiographic suspicion of Type A dissection and a significantly elevated D-dimer level, which is known to have high sensitivity but limited specificity in acute aortic syndromes [10], contrast-enhanced CT was indicated as the definitive diagnostic modality. In this patient, the clinical history yielded an Aortic Dissection Detection Risk Score (ADD-RS) of 1 [11], based on a family history of aortic disease, indicating an intermediate pre-test probability and further supporting the decision to proceed with contrast-enhanced CT of the thoracic aorta.
The initial contrast-enhanced CT scan did not confirm an acute dissection of the ascending aorta. However, image quality was limited by suboptimal contrast enhancement and obesity-related artifacts.
During the 8-hour interval between the 2 CT scans of the thoracic aorta, the patient remained hemodynamically stable and asymptomatic while receiving antihypertensive treatment. Management included a beta-blocker, an angiotensin-converting enzyme inhibitor, and intravenous nitroglycerin, with BP maintained below 110/60 mmHg. Given the inconclusive nature of the first scan and the absence of clinical deterioration, alternative diagnoses – including neurovascular and musculoskeletal causes – were considered. No additional imaging beyond echocardiography was initially performed. The early TTE findings were interpreted with caution due to their potential artifact-like appearance.
After the shift change, a follow-up TTE was conducted by a different physician, revealing a similar image that was still suspicious for Type A dissection, prompting a repeat CT scan of the thoracic aorta, which definitively confirmed the diagnosis (Figure 5).
No atherosclerotic plaques or other stenoses were identified in the coronary arteries. Both scans revealed a pathological volume of pericardial fluid with a density of 45–50 Hounsfield units, consistent with hemorrhagic effusion.
Although transesophageal echocardiography (TEE) was considered following TTE and the initial CT scan, it was ultimately deferred in favor of repeating the CT scan as a less invasive alternative. Had the repeat CT failed to confirm acute dissection of the ascending aorta, TEE would have been pursued for a definitive diagnosis.
The patient underwent immediate surgery. Intraoperatively, a tear in the aortic intima was identified 3 mm above the left coronary artery ostium. The dissection involved half the aortic circumference and extended to the level of the brachiocephalic trunk without propagating to the side branches. A large amount of blood and a clot were present in the pericardial sac.
The affected aortic segment was resected and replaced with a synthetic graft (JOTEC, Heshingen, Germany), preserving the aortic root. A pericardial hematoma was evacuated. After an uncomplicated postoperative course, the patient was discharged in good health. Genetic screening for heritable aortic conditions was recommended for the patient and his family members. Several months after surgery, the patient remained asymptomatic and continued in outpatient care; however, genetic testing had not yet been performed at the time of the writing of this report.
A visual timeline summarizing the diagnostic and therapeutic milestones is presented in Figure 6.
The authors have obtained permission from the patient for the anonymous use of his imaging and clinical data, as well as for the publication of this case report.
Discussion
LIMITATIONS AND FUTURE DIRECTIONS:
This case illustrates both the challenges and learning opportunities associated with atypical presentations of Type A AAD. The main limitation was the diagnostic delay, which resulted from the absence of classical symptoms and the suboptimal quality of the initial CT scan. Although TTE raised a suspicion of dissection, its earlier use could have potentially shortened the diagnostic pathway. Another limitation is the absence of long-term follow-up data; this absence restricts the evaluation of delayed complications, survival, and recurrence risk.
Future research should focus on assessing the diagnostic utility of sequential and complementary imaging strategies in cases with ambiguous initial findings. In addition, more data are needed on the prevalence and clinical significance of isolated neck pain as an initial manifestation of AAD. Finally, efforts to refine risk stratification tools and diagnostic algorithms by incorporating atypical symptomatology may help reduce misdiagnosis and improve early detection in high-risk patients.
Conclusions
This case report underscores isolated neck pain as an uncommon yet potentially life-threatening presentation of Stanford Type A AAD. Clinicians should consider AAD in the differential diagnosis of unexplained neck pain, particularly in patients with identifiable risk factors such as arterial hypertension or a positive family history.
Timely recognition and early use of multimodal imaging are crucial, even when classical symptoms are absent. This report contributes to the limited literature on atypical AAD presentations, emphasizing the importance of clinical vigilance for non-classical signs to enhance diagnostic accuracy and improve patient outcomes. Clinicians should maintain a high index of suspicion for AAD in high-risk patients presenting with unexplained, atypical pain, even in the absence of classical thoracic symptoms.
Figures
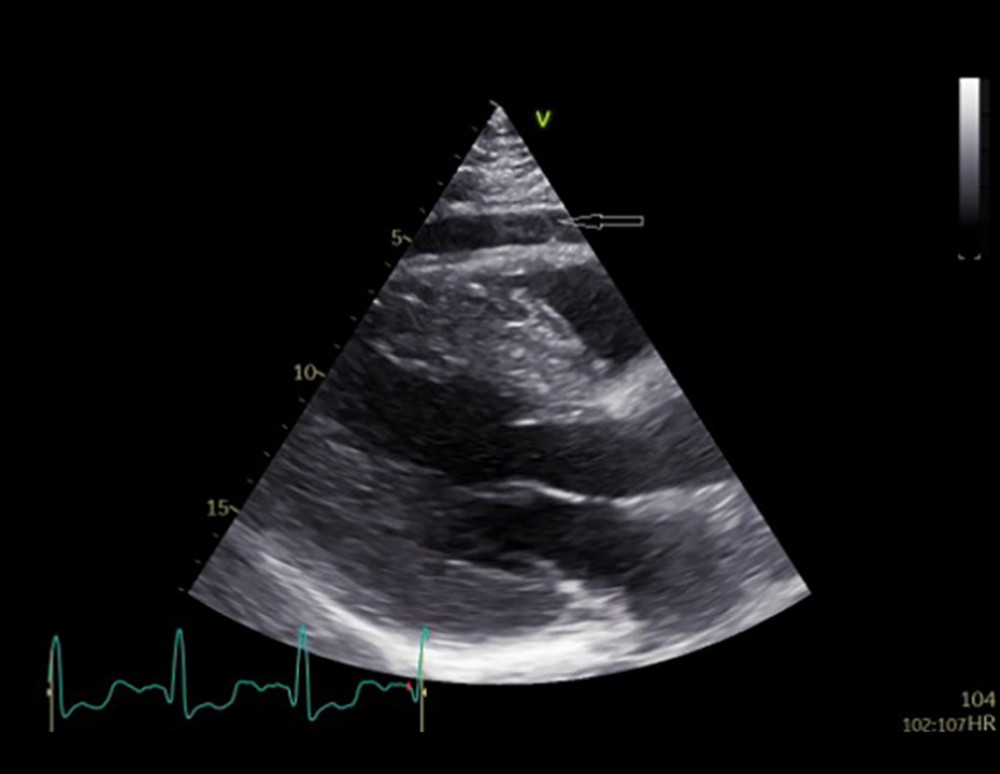 Figure 1. Two-dimensional transthoracic echocardiography. The parasternal long-axis view demonstrates left ventricular hypertrophy and regional pericardial effusion (arrow) anterior to the right ventricle.
Figure 1. Two-dimensional transthoracic echocardiography. The parasternal long-axis view demonstrates left ventricular hypertrophy and regional pericardial effusion (arrow) anterior to the right ventricle. 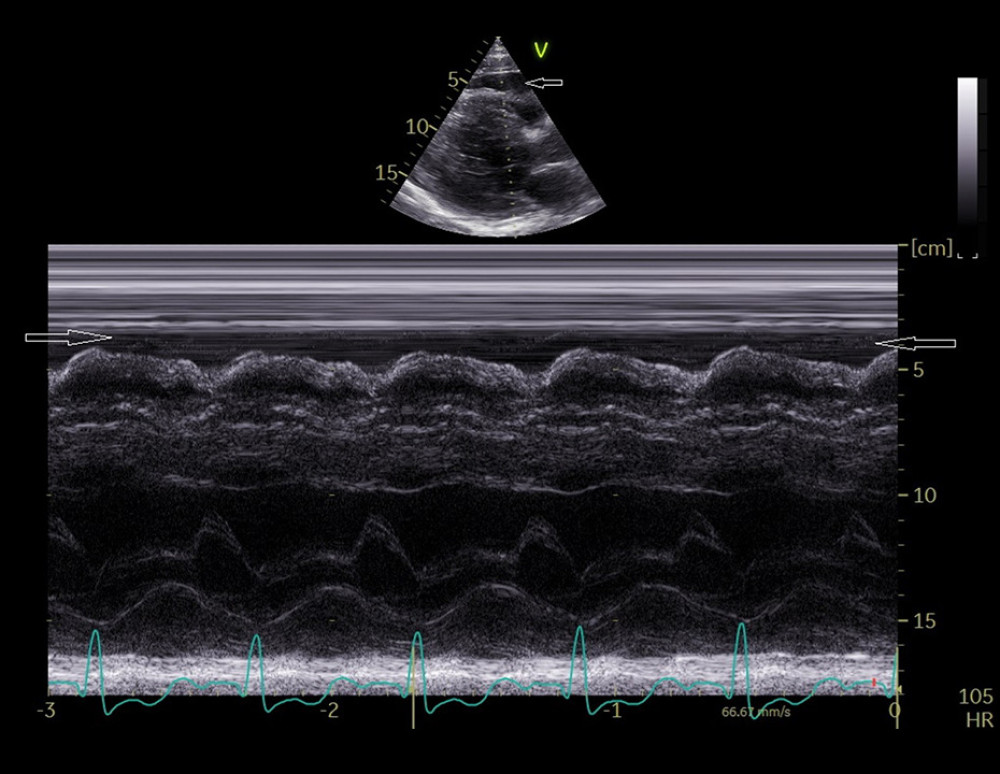 Figure 2. M-mode transthoracic echocardiography. The parasternal long-axis view shows regional pericardial effusion (arrows) anterior to the right ventricle.
Figure 2. M-mode transthoracic echocardiography. The parasternal long-axis view shows regional pericardial effusion (arrows) anterior to the right ventricle. ![Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta reveals 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicative of ascending aortic dissection extending into the proximal aortic arch.](https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e949758-g003.jpg&idArt=949758&w=1000) Figure 3. Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta reveals 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicative of ascending aortic dissection extending into the proximal aortic arch.
Figure 3. Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta reveals 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicative of ascending aortic dissection extending into the proximal aortic arch. ![Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta shows 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicating an ascending aortic dissection extending into the proximal aortic arch.](https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e949758-g004.jpg&idArt=949758&w=1000) Figure 4. Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta shows 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicating an ascending aortic dissection extending into the proximal aortic arch.
Figure 4. Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta shows 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicating an ascending aortic dissection extending into the proximal aortic arch. 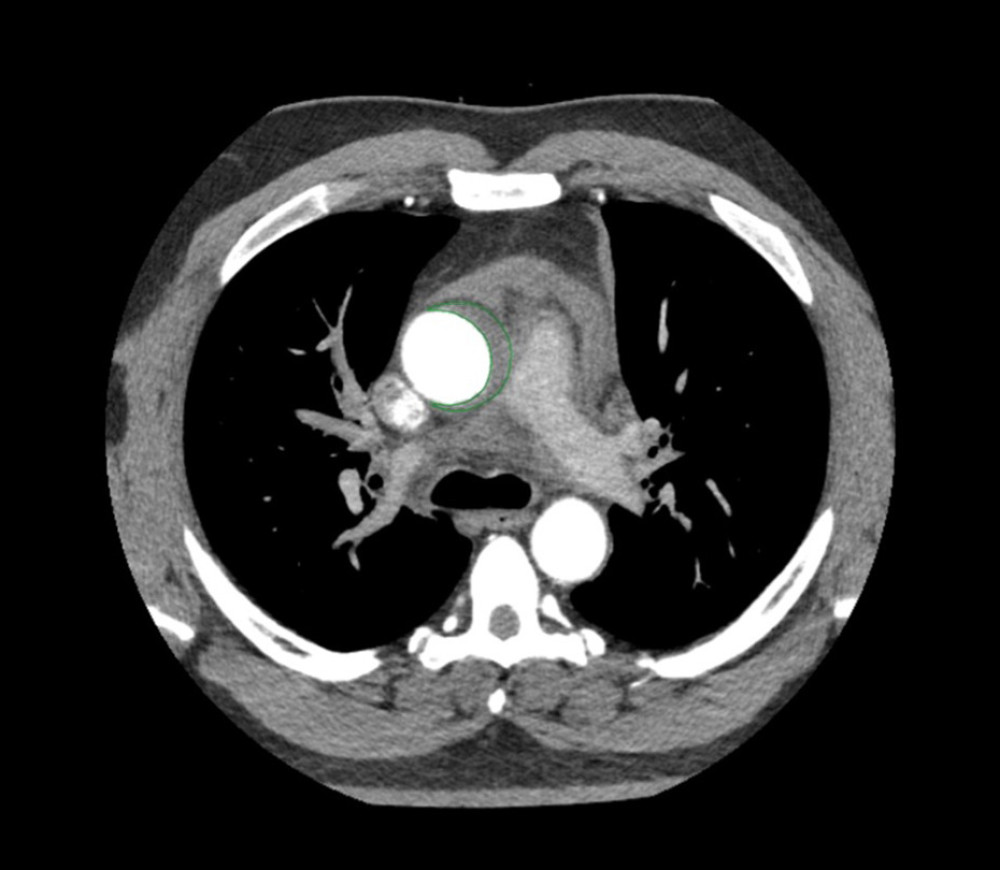 Figure 5. Contrast-enhanced computed tomography with axial reconstruction suggestive of Stanford Type A acute aortic dissection (gray region inside the green line).
Figure 5. Contrast-enhanced computed tomography with axial reconstruction suggestive of Stanford Type A acute aortic dissection (gray region inside the green line). 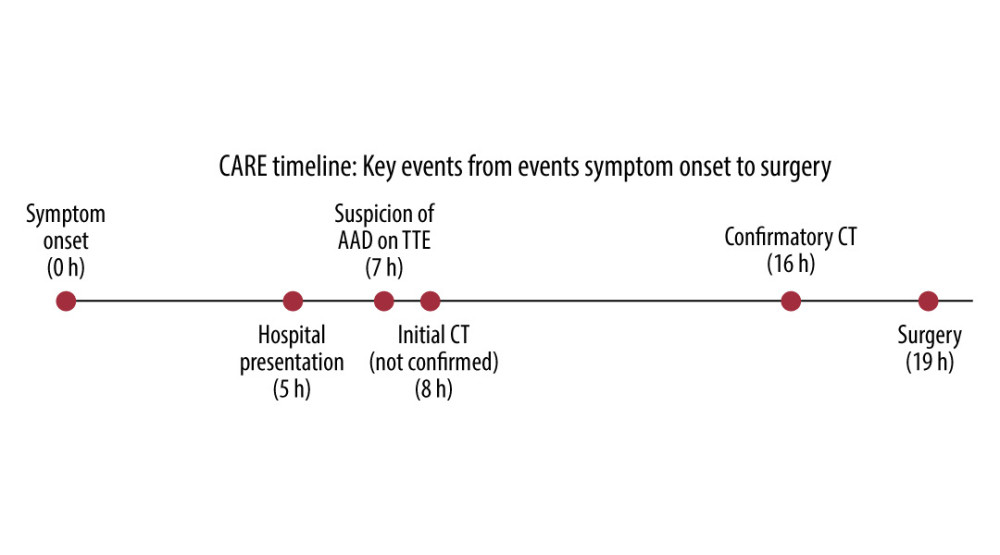 Figure 6. CARE timeline illustrating key diagnostic and therapeutic events from symptom onset to surgery. CARE – CAse REport guidelines; AAD – acute aortic dissection; TTE – transthoracic echocardiography; CT – computed tomography.
Figure 6. CARE timeline illustrating key diagnostic and therapeutic events from symptom onset to surgery. CARE – CAse REport guidelines; AAD – acute aortic dissection; TTE – transthoracic echocardiography; CT – computed tomography. References
1. Think aorta: Think aorta public information campaign [Internet], Think aorta [cited 2025 Jul 23]. Available from: https://www.thinkaorta.net
2. Erbel R, Aboyans V, Boileau C, 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC): Eur Heart J, 2014; 35; 2873-926
3. Isselbacher EM, Preventza O, Hamilton Black J, 2022 ACC/AHA Guideline for the diagnosis and management of aortic disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines: Circulation, 2022; 146; e334-e482
4. Czerny M, Grabenwöger M, Berger T, EACTS/STS guidelines for diagnosing and treating acute and chronic syndromes of the aortic organ: Ann Thorac Surg, 2024; 118; 5-115
5. Lovatt S, Wong CW, Schwarz K, Misdiagnosis of aortic dissection: A systematic review of the literature: Am J Emerg Med, 2022; 53; 16-22
6. Mazzolai L, Teixido-Tura G, Lanzi S, 2024 ESC Guidelines for the management of peripheral arterial and aortic diseases: Eur Heart J, 2024; 45; 3538-700
7. Chiu P, Miller DC, Evolution of surgical therapy for Stanford acute type A aortic dissection: Ann Cardiothorac Surg, 2016; 5; 275-95
8. Daily PO, Trueblood HW, Stinson EB, Management of acute aortic dissections: Ann Thorac Surg, 1970; 10; 237-47
9. Tsukube T, Decision making and management of acute type-A dissection presenting with shock or cardiac arrest: Asian Cardiovasc Thorac Ann, 2023; 31; 20-25
10. Essat M, Goodacre S, Pandor A, Diagnostic accuracy of D-dimer for acute aortic syndromes: Systematic review and meta-analysis: Ann Emerg Med, 2024; 84; 409-21
11. Rogers AM, Hermann LK, Booher AM, Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: Results from the international registry of acute aortic dissection: Circulation, 2011; 123; 2213-18
12. Gaul C, Dietrich W, Friedrich I, Neurological symptoms in type A aortic dissections: Stroke, 2007; 38; 292-97
13. Liao W-B, Bullard MJ, Chang C-H, Aortic dissection in Taiwan: Jpn Heart J, 1995; 36; 639-45
14. Mathys J, Lachat M, Herren T, Headache as a manifestation of a life-threatening vascular disorder: Headache, 2004; 44; 706-9
15. Silbert PL, Mokri B, Schievink WI, Headache and neck pain in spontaneous internal carotid and vertebral artery dissections: Neurology, 1995; 45; 1517-22
16. Stahmer SA, Raps EC, Mines DI, Carotid and vertebral artery dissections: Emerg Med Clin North Am, 1997; 15; 677-98
17. Myers DE, Vagus nerve pain referred to the craniofacial region. A case report and literature review with implications for referred cardiac pain: Br Dent J, 2008; 204; 187-89
18. Li CH, Hsu YC, Hsu YC, Left mandibular pain in a patient of aortic dissection presenting with acute ischemic stroke: A case report: Acta Neurol Taiwan, 2014; 23; 129-33
19. Bressler M, Klein E, Shayowitz M, A case of late diagnosis of acute aortic dissection involving the carotid arteries in a patient presenting with signs of acute ischemic stroke: Am J Case Rep, 2020; 21; e919271
20. Callaway M, Redfern E, France J: The Royal College of Emergency Medicine & The Royal College of Radiologists Best Practice Guideline: Diagnosis of thoracic aortic dissection in the Emergency Department [Internet], 2024, London, Royal College of Radiologists [cited 2025 Jul 23]; Available from: https://www.rcr.ac.uk/media/hwubc3le/diagnosis-of-thoracic-aortic-dissection-in-the-ed-_updated-march-2025.pdf
21. Mancusi C, Basile C, Fucile I, Aortic remodeling in patients with arterial hypertension: Pathophysiological mechanisms, therapeutic interventions and preventive strategies-a position paper from the Heart and Hypertension Working Group of the Italian Society of Hypertension: High Blood Press Cardiovasc Prev, 2025; 32; 255-73
22. Hibino M, Otaki Y, Kobeissi E, Blood pressure, hypertension, and the risk of aortic dissection incidence and mortality: Results from the J-SCH Study, the UK Biobank Study, and a meta-analysis of cohort studies: Circulation, 2022; 145; 633-44
23. Braverman AC, Acute aortic dissection: clinician update: Circulation, 2010; 122; 184-88
24. Hibino M, Verma S, Jarret CM, Temporal trends in mortality of aortic dissection and rupture in the UK, Japan, the USA and Canada: Heart, 2024; 110; 331-36
Figures
Figure 1. Two-dimensional transthoracic echocardiography. The parasternal long-axis view demonstrates left ventricular hypertrophy and regional pericardial effusion (arrow) anterior to the right ventricle.Figure 2. M-mode transthoracic echocardiography. The parasternal long-axis view shows regional pericardial effusion (arrows) anterior to the right ventricle.Figure 3. Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta reveals 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicative of ascending aortic dissection extending into the proximal aortic arch.Figure 4. Two-dimensional transthoracic echocardiography. The suprasternal view of the aorta shows 2 vascular lumina (true [arrow] and false [arrowhead]) separated by an intimal flap, indicating an ascending aortic dissection extending into the proximal aortic arch.Figure 5. Contrast-enhanced computed tomography with axial reconstruction suggestive of Stanford Type A acute aortic dissection (gray region inside the green line).Figure 6. CARE timeline illustrating key diagnostic and therapeutic events from symptom onset to surgery. CARE – CAse REport guidelines; AAD – acute aortic dissection; TTE – transthoracic echocardiography; CT – computed tomography. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.949976
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950290
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950607
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950985
Most Viewed Current Articles
07 Dec 2021 : Case report  17,691,734
17,691,734
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  164,491
164,491
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
113,090
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
59,175
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133