25 December 2025: Articles 
Guillain-Barré Syndrome in the Third Trimester of Pregnancy: A Case Report and Literature Review
Rare disease
Liang Gao ABCDEF 1, Mouchang Qiu BF 1, Hua Qian ADE 1*DOI: 10.12659/AJCR.949852
Am J Case Rep 2025; 26:e949852






Abstract
BACKGROUND: Guillain-Barré syndrome (GBS) is a rare autoimmune peripheral neuropathy. Its hallmark features include rapidly progressive muscle weakness and areflexia. This report describes a 34-year-old woman in the third trimester of pregnancy who presented with limb weakness and was diagnosed with GBS. The patient underwent treatment with intravenous immunoglobulin (IVIG) and high-dose corticosteroid therapy.
CASE REPORT: A 34-year-old pregnant woman developed bilateral limb weakness at 36 weeks of gestation. Upon hospital admission and clinical evaluation, multidisciplinary consultation was conducted. Considering her history of diarrhea 1 week earlier, the presence of dyspnea, bilateral limb muscle weakness, physical examination findings of decreased muscle strength and diminished deep tendon reflexes with preserved limb sensation, GBS was suspected as the primary diagnosis. As her condition continued to deteriorate, she underwent an emergency cesarean delivery under spinal anesthesia. Postoperatively, her muscle weakness progressively worsened. IVIG and high-dose corticosteroid therapy was initiated, resulting in significant clinical improvement. Both mother and infant were subsequently discharged to a local hospital for continued rehabilitation.
CONCLUSIONS: This case underscores the dynamic progression of GBS, particularly in obstetric populations, and emphasizes the critical role of early recognition and multidisciplinary collaboration in optimizing maternal and neonatal outcomes. The report aims to enhance clinical awareness, improve diagnostic accuracy, and inform therapeutic strategies for similar cases.
Keywords: Pregnancy Trimester, Third, Syndrome, Motor Disorders, Humans, Female, Pregnancy, Guillain-Barré syndrome, adult, Pregnancy Complications, Immunoglobulins, Intravenous, Cesarean Section
Introduction
Guillain-Barré syndrome (GBS) is an acute or subacute peripheral nerve disorder caused by the immune system abnormally damaging nerve myelin sheaths or axons [1]. Viral infections serve as significant triggers for GBS [2]. GBS typically manifests as symmetric weakness and sensory abnormalities in the distal lower limbs. As the condition progresses, respiratory muscle weakness can develop, potentially leading to paralysis and ultimately respiratory failure [3]. GBS can occur at any stage of pregnancy or the postpartum period, most commonly during the third trimester and within the first 2 weeks postpartum [4,5]. GBS is rare in pregnancy, and its nonspecific clinical manifestations pose significant diagnostic challenges, necessitating differentiation from other pregnancy-related neurological complications. The overlap between physiological changes in pregnancy and early manifestations of GBS can obscure timely recognition, while treatment decisions must carefully balance maternal safety and fetal well-being.
This case report underscores the diagnostic complexities of GBS in obstetric settings, in which its nonspecific symptomatology often leads to delayed recognition. Multidisciplinary collaboration among maternal-fetal medicine specialists, neuroimmunologists, and critical care teams is imperative to mitigate maternal and fetal risks associated with diagnostic delays.
Case Report
A 34-year-old pregnant woman at 36 weeks and 3 days of gestation was transferred to our obstetrics department from a local hospital due to 12 hours of progressive limb weakness. The patient had experienced diarrhea 1 week prior. Twelve hours before admission, she developed delayed responsiveness and generalized weakness. There were no prior autoimmune disorders, allergies, or family history of neuropathy. Mild anemia had been diagnosed during the second trimester of pregnancy and was managed with oral iron supplementation. The patient had not undergone regular prenatal check-ups. Upon admission, she was conscious but lethargic, with mild tachypnea. Initial laboratory test results and obstetric ultrasound were unremarkable. Electromyography revealed partial motor conduction block in the motor nerves. Neurological consultation revealed a conscious patient with slowed mentation, exhibiting Grade III muscle strength in the upper limbs and Grade II in the lower limbs, diminished tendon reflexes, intact sensory function, and absence of pathological signs. Because of respiratory deterioration, an emergency cesarean delivery under combined spinal-epidural anesthesia was performed, delivering a mature female infant weighing 2.910 g, with Apgar scores of 8 and 9 at 1 minute and 5 minutes, respectively. The neonate was transferred to the neonatal intensive care unit, and the mother was admitted to the intensive care unit for neurosupportive management. Postoperatively, the patient experienced further weakness. Following neurology consultation, she received intravenous immunoglobulin (IVIG) at 0.4 g/kg/day for 5 days; Concurrently, empirical treatment with methylprednisolone was administered intravenously at a dose of 240 mg per day for 5 consecutive days, followed by a tapering protocol. Adjunctive therapies included fursultiamine (50 mg 3 times daily), mecobalamin (0.5 mg 3 times daily), and Ginkgo biloba extract (0.15 g 3 times daily). By the second day of IVIG therapy, muscle strength of the patient improved. On postoperative day 4, Neurological examination revealed upper limb strength of grade IV, lower limb strength of grade III, intact sensation, mildly diminished tendon reflexes, and absent pathological signs. She was discharged on postoperative day 8 to a local hospital for continued rehabilitation. At the 6-week postpartum follow-up, she had achieved complete neurological recovery. This case highlights the importance of early recognition, multidisciplinary collaboration, and prompt immunotherapy in managing GBS during pregnancy, to ultimately ensure favorable maternal and neonatal outcomes.
Discussion
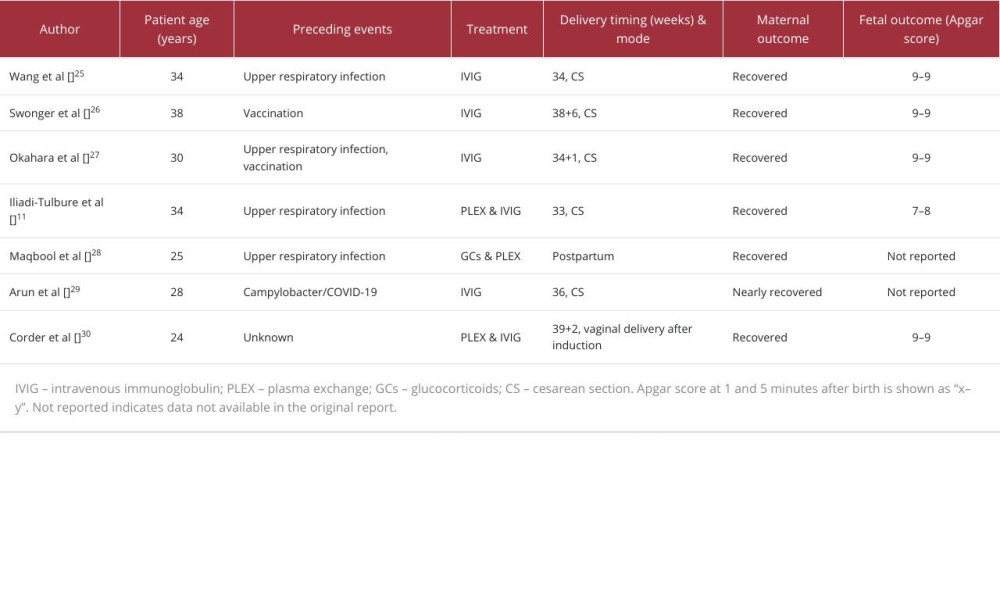
To contextualize the present case, we conducted a narrative review of the literature. A literature search was performed in PubMed and Web of Science databases using the keywords “Guillain-Barré syndrome” and “pregnancy”. Articles published in English between January 2010 and March 2025 were considered. We included case reports, case series, and relevant reviews that discussed the clinical presentation, diagnosis, treatment, and maternal or neonatal outcomes of GBS during pregnancy (Table 1). References were further screened from the bibliographies of the retrieved articles to ensure comprehensive coverage.
Epidemiological studies indicate that the annual incidence of GBS in the general population ranges from 0.75 to 2.00 per 100 000 individuals [6]. Notably, a study identified 291 GBS cases among 13 792 544 pregnant individuals in a nationwide cohort, yielding an incidence rate of 2.1 per 100 000 deliveries [7]. These findings suggest no statistically significant elevation in GBS incidence during pregnancy, compared with the general population, which showed that gestation itself does not confer an additional risk for GBS development. Clinically GBS subtypes are categorized as classic variants – acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), and acute motor-sensory axonal neuropathy – and atypical variants, which include rare clinical phenotypes. Geographical heterogeneity exists in subtype prevalence: AMAN predominates in China and other Asian countries, whereas AIDP is more common in Western populations [3,8,9]. This epidemiological divergence may reflect region-specific interactions between environmental triggers and host genetic factors, including polymorphisms in HLA class II alleles and ganglioside antibody production patterns [10]. Such variations potentially influence not only disease subtypes but also clinical trajectories and severity outcomes.
While the precise etiology of GBS remains incompletely elucidated, approximately 70% of cases are preceded by viral or bacterial infections. Molecular mimicry-driven cross-reactivity between microbial antigens and peripheral nerve components underlies this post-infectious autoimmune process [11].
The diagnosis of GBS is established through comprehensive evaluation integrating medical history, clinical manifestations, neurological examinations, cerebrospinal fluid (CSF) analysis, and electrophysiological studies [15]. Mandatory diagnostic criteria include (1) acute onset with disease progression generally not exceeding 4 weeks, followed by stabilization or improvement; and (2) clinical features consistent with classic GBS or its variants. CSF albuminocytological dissociation (elevated protein levels with normal cell counts), a characteristic finding peaking at 2 to 4 weeks after onset, is absent in 20% to 30% of mild cases. Electrophysiological studies confirm peripheral neuropathy, differentiate demyelinating from axonal damage, and aid subtyping, although results vary significantly across subtypes, disease stages, and severity levels, with normal findings common in early phases (<7 days). Therefore, the inherent delay in supportive diagnostic confirmation of GBS underscores the critical importance of early intervention in pregnant patients to effectively reduce maternal-fetal risks. Differential diagnoses include immune-mediated disorders, such as encephalomyelitis and autoimmune nodopathies; infectious etiologies, such as poliomyelitis, Lyme disease, and brucellosis-related neuropathy; and neuromuscular conditions, such as myasthenia gravis, periodic paralysis, and acute rhabdomyolysis.
The management of GBS during pregnancy aligns with standard protocols for the general population but requires coordinated multidisciplinary care involving obstetricians, neurologists, anesthesiologists, and rehabilitation specialists. Early initiation of immunotherapy after diagnosis is critical to halt disease progression and minimize disability [16]. IVIG and plasma exchange (PLEX) are first-line immunotherapies, having demonstrated equivalent efficacy [17,18]. For pregnant patients, IVIG is preferred because of its favorable safety profile, with no dose adjustment required and no evidence of fetal teratogenicity [5,15]. In contrast, PLEX necessitates rigorous hemodynamic monitoring, as hypotension during treatment can compromise placental perfusion, potentially triggering fetal distress [19]. This risk is substantially mitigated by adequate volume resuscitation prior to PLEX [20]. Additionally, gestational plasma volume expansion is frequently underestimated during PLEX, leading to suboptimal exchange volumes and reduced therapeutic efficacy [21]. Thus, meticulous fluid management and real-time hemodynamic surveillance are mandatory for pregnant patients with GBS undergoing PLEX.
Multiple clinical trials have demonstrated that glucocorticoid monotherapy lacks definitive therapeutic efficacy in GBS, with no significant difference observed between combined glucocorticoid/IVIG regimens and IVIG alone. In a systematic review that included multiple randomized controlled trials or quasi-randomized controlled trials comparing corticosteroids or adrenocorticotropic hormone with placebo or supportive care alone in patients with GBS, moderate-quality evidence indicated that corticosteroid monotherapy did not significantly accelerate recovery or affect long-term outcomes [22]. Notably, clinical cohorts have shown that high-dose glucocorticoids pose significant risks during pregnancy, including cleft palate malformations. Additionally, glucocorticoids induce maternal glucose and lipid metabolism disturbances, increasing risks of fetal intrauterine growth restriction, preterm delivery, and neonatal complications [23]. Consequently, glucocorticoids are not recommended as standard therapy for GBS, particularly during pregnancy.
Respiratory and swallowing function assessments are critical priorities in GBS management, with early recognition of respiratory compromise and dysphagia being pivotal for improving outcomes. After stabilization, neurorehabilitation protocols should commence within 72 hours to mitigate disuse muscle atrophy and prevent joint contractures. Therapeutic decisions must integrate gestational age, maternal-fetal status, and fetal lung maturity, with delivery timing and mode determined by maternal neurological stability and fetal biophysical profiles. Puerperal management aligns with general population protocols, although lactation requires IVIG pharmacokinetic considerations.
GBS exhibits significant clinical heterogeneity, leading to considerable variability in patient prognoses. GBS typically follows a self-limiting, monophasic course, with disease progression ceasing within 4 weeks of onset, and functional recovery occurring over weeks to months. Relapse is rare. While most patients achieve complete recovery or retain only mild neurological deficits, approximately 3% to 5% die from complications such as respiratory failure, fatal arrhythmias, pneumothorax, sepsis, or pulmonary embolism [5]. Notably, 10% of survivors develop significant residual disability, and 3% progress to have chronic inflammatory demyelinating polyneuropathy. Advances in critical care have markedly improved outcomes in pregnancy-associated GBS, with mortality declining from 33%, to 1–5% in contemporary cohorts; however, 10% to 20% of patients still experience severe disability [11]. Poor prognostic indicators include rapid progression to mechanical ventilation within 7 days, motor action potential amplitudes less than 20% of normal, and extensive denervation on electromyography. The Erasmus Guillain-Barré Outcome Score is used to assess the prognosis of this condition [24]; however, its accuracy requires further validation.
In the presented case, the patient had a recent history of gastrointestinal infection (1 week prior) and acute-onset progressive limb weakness. Multidisciplinary evaluation strongly suggested GBS (likely the AMAN subtype), prompting emergency cesarean delivery under spinal anesthesia. Although CSF analysis during spinal anesthesia could have provided more definitive diagnostic confirmation, it was not performed in this case. This omission occurred because the importance of the procedure was not sufficiently communicated to the patient and her family, and preoperative informed consent was therefore not obtained. While the absence of CSF analysis represents a limitation, the combination of clinical findings and electrophysiological evidence still provided a solid basis for establishing the diagnosis.
Postoperatively, the patient exhibited progressive neuromuscular deterioration. Following multidisciplinary consultation, we initiated a treatment regimen of high-dose glucocorticoids combined with IVIG, and neurotrophic therapy was administered. This decision was primarily based on local clinical practice patterns and the attending neurologist’s prior experience in managing GBS. However, with the accumulation of research evidence and the release of updated international guidelines, the use of glucocorticoids either alone or in combination with IVIG is no longer recommended, as it offers no additional therapeutic benefit and can increase risks for both mother and infant. This case highlights the importance of aligning clinical decision-making with the most up-to-date evidence-based guidelines, and our team will adhere to these recommendations in future cases.
The patient ultimately achieved symptomatic improvement. At the 6-week postpartum follow-up, complete neurological recovery was documented, with no residual complications.
Conclusions
GBS is a rare peripheral neurological disorder in pregnancy that is strongly associated with enteroviral infections. Its nonspecific early manifestations necessitate heightened clinical vigilance. Timely diagnosis, aggressive intervention, and proactive management of perinatal complications are critical for optimizing maternal and fetal outcomes.
References
1. Leonhard SE, Mandarakas MR, Gondim FAA, Diagnosis and management of Guillain-Barré syndrome in ten steps: Nat Rev Neurol, 2019; 15(11); 671-83
2. Wachira VK, Farinasso CM, Silva RB, Peixoto HM, de Oliveira MRF, Incidence of Guillain-Barré syndrome in the world between 1985 and 2020: A systematic review: Glob Epidemiol, 2023; 5; 100098
3. Fokke C, van den Berg B, Drenthen J, Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria: Brain, 2014; 137(Pt 1); 33-43
4. Campos da Silva F, de Moraes Paula G, Dos Santos Esteves Automari CV, Guillain-Barré syndrome in pregnancy: Early diagnosis and treatment is essential for a favorable outcome: Gynecol Obstet Invest, 2009; 67(4); 236-37
5. Patra AK, Das M, Choudhury SS, Outcome of Guillain-Barré syndrome (GBS) during peripartum period: A hospital-based observational study: Ann Indian Acad Neurol, 2022; 25(3); 417-21
6. Sejvar JJ, Baughman AL, Wise M, Morgan OW, Population incidence of Guillain-Barré syndrome: A systematic review and meta-analysis: Neuroepidemiology, 2011; 36(2); 123-33
7. Taylor S, Czuzoj-Shulman N, Spence AR, Abenhaim HA, Maternal and newborn outcomes in pregnancies complicated by Guillain-Barré syndrome: J Perinat Med, 2024; 52(8); 870-77
8. Wakerley BR, Uncini A, Yuki NGBS Classification Group; GBS Classification Group, Guillain-Barré and Miller Fisher syndromes – new diagnostic classification: Nat Rev Neurol, 2014; 10(9); 537-44 [Erratum in: Nat Rev Neurol. 2014;10(11):612]
9. Tan CY, Razali SNO, Goh KJ, Shahrizaila N, Diagnosis of Guillain-Barré syndrome and validation of the Brighton criteria in Malaysia: J Peripher Nerv Syst, 2020; 25(3); 256-64
10. Dimachkie MM, Barohn RJ, Guillain-Barré syndrome and variants: Neurol Clin, 2013; 31(2); 491-510
11. Iliadi-Tulbure C, Cemortan M, Jubirca S, Guillain-Barré syndrome in pregnancy: A case report and review of the literature: AJOG Glob Rep, 2024; 4(4); 100396
12. de Andrade da Silva R, Cremaschi RC, Rebello Pinho JR, Guillain-Barré syndrome – the challenge of unrecognized triggers: Neurol Sci, 2019; 40(11); 2403-4
13. Araujo Coelho DR, Melo Mendes IC, Guillain-Barré syndrome and encephalitis following a cytomegalovirus infection in an immunocompetent adult: A case report: Am J Case Rep, 2024; 25; e944337
14. Ferreira SDC, Vasconcelos JRO, Rezende REF, Guillain-Barré syndrome in a patient receiving anti-tumor necrosis factor for Crohn disease: Coincidence or consequence?: Am J Case Rep, 2024; 25; e943709
15. Pacheco LD, Saad AF, Hankins GD, Guillain-Barré syndrome in pregnancy: Obstet Gynecol, 2016; 128(5); 1105-10
16. Yamagishi Y, Suzuki H, Sonoo M, Markers for Guillain-Barré syndrome with poor prognosis: A multi-center study: J Peripher Nerv Syst, 2017; 22(4); 433-39
17. Doets AY, Jacobs BC, van Doorn PA, Advances in management of Guillain-Barré syndrome: Curr Opin Neurol, 2018; 31(5); 541-50
18. Khaja M, Gomez GPR, Santana Y, A 44-year-old Hispanic man with loss of taste and bilateral facial weakness diagnosed with Guillain-Barré syndrome and Bell’s palsy associated with SARS-CoV-2 infection treated with intravenous immunoglobulin: Am J Case Rep, 2020; 21; e927956
19. Colpo A, Marson P, Pavanello F, Therapeutic apheresis during pregnancy: A single center experience: Transfus Apher Sci, 2019; 58(5); 652-58
20. Ogura M, Makino H, Kamiya C, Lipoprotein apheresis is essential for managing pregnancies in patients with homozygous familial hypercholesterolemia: Seven case series and discussion: Atherosclerosis, 2016; 254; 179-83
21. Cox JL, Koepsell SA, Shunkwiler SM, Therapeutic plasma exchange and pregnancy: A case report and guidelines for performing plasma exchange in a pregnant patient: J Clin Apher, 2017; 32(3); 191-95
22. Hughes RA, Brassington R, Gunn AA, van Doorn PA, Corticosteroids for Guillain-Barré syndrome: Cochrane Database Syst Rev, 2016; 10(10); CD001446
23. Marazita ML, Genexenvironment associations in orofacial clefting: Curr Top Dev Biol, 2023; 152; 169-92
24. Busl KM, Fried H, Muehlschlegel S, Guidelines for neuroprognostication in adults with Guillain-Barré syndrome: Neurocrit Care, 2023; 38(3); 564-83
25. Wang J, Bahabri A, Wong P, Anantharachagan A, An atypical presentation of pre-eclampsia (PET) in a patient diagnosed with Guillain-Barré syndrome: A case report: Case Rep Womens Health, 2023; 37; e00489
26. Swonger RM, Syros A, Finch L, Guillain-Barré syndrome with concomitant severe preeclampsia: A case report: Cureus, 2023; 15(6); e40796
27. Okahara S, Bowe R, Wong P, Johnson M, Caesarean section for a primipara with Guillain-Barré syndrome under combined spinal epidural anaesthesia: BMJ Case Rep, 2024; 17(6); e260285
28. Maqbool M, Deekshitha K, Chandana DD, Postpartum Guillain-Barré syndrome presenting as acute motor axonal neuropathy in a young female: A report of a rare case: Cureus, 2024; 16(10); e70787
29. Arun TC, Takoor S, Ramchandani S, Supraglottic airway device in a patient with Guillain-Barré syndrome undergoing lower-segment cesarean section (LSCS): A case report: Cureus, 2025; 17(1); e77263
30. Corder VK, Collins BS, Smith T, Onset of Guillain-Barré Syndrome in a pregnant woman: A report of a rare occurrence: Cureus, 2025; 17(1); e77715
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133