31 December 2025: Articles 
Anesthetic Management of a 32-Year-Old Woman Undergoing Laparoscopic Gynecological Surgery With Prior Fontan Repair for a Complex Congenital Heart Defect
Unusual setting of medical care, Congenital defects / diseases
Stefano CatarciDOI: 10.12659/AJCR.950027
Am J Case Rep 2025; 26:e950027






Abstract
BACKGROUND: Fontan repair in complex congenital heart conditions involves creating a total cavopulmonary connection, redirecting systemic venous blood to the pulmonary circulation, and bypassing cardiac systemic blood flow. Anesthetic management for a patient with a Fontan circulation requires ensuring adequate preload and avoiding circulatory complications. This report describes the anesthetic management of a 32-year-old woman undergoing laparoscopic surgery with a history of Fontan repair of a complex congenital heart defect.
CASE REPORT: A 32-year-old woman with transposition of the great arteries, hypoplastic right ventricle, tricuspid atresia, and non-communicating vena cavae underwent Fontan repair at 12 months of age (total cavopulmonary connection with extracardiac conduit). She presented for laparoscopy for suspected ovarian cancer. Preoperative cardiac magnetic resonance imaging revealed Fontan conduit patency and borderline systemic ventricular function. Anesthetic management included advanced monitoring (FloTrac-derived cardiac index, stroke volume, stroke volume variation), tailored induction with slow titration of propofol, ventilation with low tidal volumes and zero positive end-expiratory pressure, and vigilant fluid management. During pneumoperitoneum (12 mmHg), decreased stroke volume and mean arterial pressure were corrected with fluid boluses. At the end of surgery, the patient was extubated uneventfully and monitored in the postoperative intensive care unit for 36 hours.
CONCLUSIONS: Laparoscopic surgery in patients with Fontan circulation poses significant anesthetic challenges. This case highlights the importance of ensuring adequate preload, minimizing pulmonary vascular resistance, maintaining low intra-abdominal pressure, and using advanced hemodynamic monitoring to guarantee perioperative safety.
Keywords: Anesthesia, Fontan Procedure, Gynecologic Surgical Procedures, Hemodynamic Monitoring, Laparoscopy, univentricular heart, Humans, Female, adult, Heart Defects, Congenital
Introduction
Adult patients with congenital heart disease constitute a growing population, primarily due to advances in surgical techniques and improved long-term survival. Consequently, noncardiac surgeries in this complex group are becoming an increasingly important concern for anesthesiologists. Among these patients, individuals with single ventricle physiology who have undergone Fontan palliation make up a particularly high-risk subset in the perioperative setting. The unique hemodynamic characteristics of Fontan circulation pose significant challenges for anesthesiologists, especially during laparoscopic procedures, as these patients are susceptible to various complications related to their altered cardiovascular physiology [1].
The Fontan procedure involves creating a total cavopulmonary connection, redirecting systemic venous blood to the pulmonary circulation, and bypassing the heart [2]. This staged approach reduces the workload on the single ventricle, allowing it to focus on systemic circulation. While the Fontan procedure significantly improves survival and quality of life, it is associated with long-term complications, including increased systemic venous pressure, arrhythmias, and risks related to pulmonary vascular resistance [2]. This physiology totally depends on a low pulmonary vascular resistance and adequate preload [1,2]. Indeed, the passive flow relies on a pressure gradient between the systemic veins and the pulmonary capillary bed. As a result, any condition that increases pulmonary vascular resistance (eg, hypercapnia, hypoxia, acidosis) or impairs venous return (eg, elevated intrathoracic, intra-abdominal pressure) can significantly compromise cardiac output [3].
Moreover, laparoscopic surgery can profoundly affect venous return and pulmonary vascular resistance, particularly in patients with altered cardiopulmonary physiology, such as those with Fontan circulation. The creation of pneumoperitoneum increases intra-abdominal pressure, which can compress the inferior vena cava and splanchnic vasculature; this mechanical effect reduces venous return to the heart. While healthy individuals typically tolerate this reduction, patients with Fontan physiology, who rely on passive venous return to the pulmonary circulation, are highly preload-dependent and can experience critical reductions in cardiac output [4]. Patient positioning further influences venous return. The Trendelenburg position can transiently enhance venous return by elevating central venous pressure, whereas the reverse Trendelenburg position can exacerbate hypotension by reducing venous return, particularly in preload-sensitive patients [4,5].
Pneumoperitoneum also contributes to elevated pulmonary vascular resistance. CO2 absorption can lead to hypercapnia and respiratory acidosis, both of which increase pulmonary vascular resistance. This is particularly deleterious in patients with Fontan physiology, whose non-pulsatile pulmonary blood flow is extremely sensitive to even modest increases in pulmonary vascular resistance [4].
In addition, the effects of mechanical ventilation during general anesthesia must be carefully considered in these patients. Positive pressure ventilation increases intrathoracic pressure, which can impede pulmonary blood flow and further elevate pulmonary vascular resistance. The use of high tidal volumes and positive end-expiratory pressure can amplify these effects [4].
We present the clinical case of a patient with Fontan physiology who underwent laparoscopic oophorectomy and hysteroscopy. Some case reports have described laparoscopic surgery in adult Fontan patients, but evidence remains limited [6–11]. This report presents the anesthetic management of a woman with Fontan circulation undergoing laparoscopic gynecological surgery, highlighting clinical challenges and practical strategies.
Case Report
A 32-year-old woman with a history of complex congenital heart disease, including transposition of the great arteries, right ventricular hypoplasia, non-communicating superior and inferior vena cava, and tricuspid atresia, had previously undergone Fontan surgery at 12 months of age, consisting of a superior vena cava to right pulmonary artery connection and an inferior vena cava to right pulmonary artery conduit (Figure 1).
After undergoing the Fontan procedure, the patient developed severe subaortic stenosis, necessitating 2 further surgical interventions: resection of the infundibular septum and muscular bands through a right ventriculotomy at 6 years of age, and a Dor ventricular plasty at 19 years of age.
At the time of admission to our tertiary care center, the patient was scheduled for laparoscopic surgery for adnexal masses identified on magnetic resonance imaging (MRI) and consistent with ovarian cancer.
Upon admission, her height was 155 cm and weight 85 kg, resulting in a body mass index of 35.4 kg/m2. The patient was receiving oral acetylsalicylic acid (100 mg daily).
A multidisciplinary preoperative evaluation was conducted by a team including cardiologists, gynecologists, anesthesiologists, and cardiac surgeons. The laparoscopic approach was selected by the multidisciplinary team after considering the patient’s body mass index, the potential risk of laparotomic complications, including infection, wound dehiscence, and delayed postoperative mobilization, and the limited cardiac functional reserve.
Physical examination revealed a good general condition and normal respiratory function in both the standing and supine positions. Oxygen saturation on ambient air ranged from 92% to 94%. A treadmill stress test demonstrated reduced exercise tolerance due to deconditioning, with a sinus tachycardic response at low workload.
Cardiac MRI (Figure 2) revealed no discrete stenoses within the Fontan circuit or pulmonary arteries, with near-normal pulmonary blood flow distribution (right pulmonary artery/left pulmonary artery: 55%/45%). Systemic-to-pulmonary collateral circulation accounted for 14% of pulmonary venous return, predominantly directed to the right side, including a prominent veno-venous collateral between the azygos vein and right pulmonary vein. A functionally single ventricle of normal size (end-diastolic volume index: 73 mL/m2) was observed, with borderline systolic function (ejection fraction: 52%). No significant stenosis or regurgitation was noted in the systemic outflow tract; mild mitral regurgitation was present. Transthoracic echocardiography showed preserved left ventricular function, mild mitral regurgitation, no obstruction to aortic outflow, and laminar flow through the Fontan circuit.
Abdominopelvic MRI identified 2 contiguous right adnexal masses adjacent to the cecum and terminal ileum, with a small volume of free fluid in the pelvic cavity. Hepatomegaly, ectasia of the hepatic veins, and inferior vena cava dilation were suggestive of chronic venous outflow impairment.
The patient was classified as American Society of Anesthe-siologists Physical Status III and New York Heart Association Functional Class II.
The day of the surgery, upon arrival in the pre-anesthesia area, two 16-gauge peripheral venous lines and one 20-gauge arterial line were inserted. Premedication with 2 mg of intravenous midazolam was administered. Two units of red blood cells were prepared in advance and made available in the operating room.
Multiparameter monitoring included electrocardiography, pulse oximetry (SpO2), bispectral index, invasive arterial pressure, and urine output. Additionally, we opted for minimally invasive hemodynamic monitoring to guide fluid management: the FloTrac system (Edwards Lifesciences) continuously monitored cardiac index, stroke volume (SV), and stroke volume variation (SVV) as indicators of intraoperative hemodynamics.
Baseline vital signs were blood pressure 141/86 mmHg, heart rate 80 beats/min, respiratory rate 15 breaths/min, and SpO2 92% to 94%, with a 5% increase following administration of 100% oxygen via face mask at 4 L/min.
Before induction, the patient was given 500 mL of Ringer’s lactate solution. Anesthesia induction included 15 mcg of sufentanil, slow intravenous propofol administration at 2 mg/kg over 60 seconds, and rocuronium at 0.6 mg/kg. Endotracheal intubation was performed using a 7.0-mm internal diameter tube. Mechanical ventilation was initiated with 0 cmH2O positive end-expiratory pressure, tidal volume of 6 mL/kg, and a respiratory rate adjusted between 12 and 18 breaths/min to maintain end-tidal CO2 between 30 and 35 mmHg. The fraction of inspired oxygen ranged from 0.35 to 0.4, targeting oxygen saturation above 96%.
General anesthesia was maintained with sevoflurane, titrated to achieve a minimum alveolar concentration between 1.0 and 1.5. An additional 35 mcg of sufentanil was administered before skin incision.
The patient was gradually positioned in a 15° Trendelenburg tilt at the beginning of laparoscopy to optimize surgical exposure.
Table 1 and Figure 3 show hemodynamic data recorded at baseline, at surgical incision, at pneumoperitoneum, during surgery, at the end of surgery, and upon awakening. The patient demonstrated good responsiveness to fluid loading. In the operating room, at the induction of general anesthesia, the SVV was 9%.
At the pneumoperitoneum, relative hypovolemia led to a decrease in SV, resulting in a reduced mean arterial pressure (Figure 3). Administration of an additional crystalloid bolus (1000 mL over 20 minutes) subsequently restored the baseline mean arterial pressure.
During maintenance, boluses of phenylephrine (up to 150 mcg) and ephedrine (up to 25 mg) were administered in response to cardiac index and SVV trends. Diluted norepinephrine and dobutamine infusions were prepared but not required.
A total of 2500 mL of Ringer’s lactate was administered intraoperatively. Crystalloid infusion was started before induction and continued, guided by hemodynamic parameters. Arterial blood gas analysis was performed periodically to prevent acidosis, hypercapnia, and hypoxia (Table 1).
The surgical procedure included a hysteroscopic biopsy, laparoscopic removal of adnexal masses, and omental biopsies. The total surgical duration was 77 minutes, with an estimated blood loss of 300 mL.
After awakening in the operating room, the patient was monitored in the intensive care unit for 36 hours. Postoperative analgesia was managed using a multimodal approach: acetaminophen 1 g every 6 hours, ketorolac 30 mg twice daily, and tramadol 100 mg as rescue analgesia for the first 48 postoperative hours. The patient received 2 total tramadol administrations within 48 hours for pain reported as greater than 4 on the numeric rating scale.
Discussion
This case illustrates anesthetic challenges in Fontan physiology during laparoscopic surgery: it highlights the importance of using advanced hemodynamic monitoring to ensure perioperative safety. Key lessons include optimizing preload, minimizing pulmonary vascular resistance, avoiding hypercapnia, hypoxia, and acidosis, and carefully using pneumoperitoneum pressures. SVV trends proved useful but must be interpreted cautiously.
This case contributes to the limited literature on laparoscopic surgery in patients with Fontan physiology, reinforcing that safe perioperative management is achievable with tailored strategies.
Actually, as the population of patients with univentricular hearts age, an increasing number of individuals with Fontan circulation are presenting for noncardiac surgeries, including laparoscopic procedures. However, the combination of altered cardiovascular physiology and the physiologic challenges of laparoscopy, such as pneumoperitoneum, CO2 absorption, and positional changes, can result in rapid and potentially life-threatening hemodynamic instability [3–5]. Therefore, anesthesiologists should be acutely aware of the complex interplay between Fontan physiology and anesthetic interventions, to ensure safe perioperative management.
A comprehensive, multidisciplinary preoperative evaluation is recommended and should include advanced imaging, such as echocardiography or cardiac MRI, to assess systemic ventricular function, Fontan conduit patency, the presence and significance of fenestrations, atrioventricular valve competence, and arrhythmic burden [5]. Additional considerations should include the evaluation of Fontan-associated liver disease, a common long-term complication stemming from chronic hepatic congestion and low cardiac output [12]. Hemoglobin concentration and coagulation status should also be assessed, given the frequent use of long-term antithrombotic therapy and the inherent prothrombotic state in patients with Fontan circulation [5].
In our case, a laparoscopic approach was selected, as it was considered the most appropriate surgical option to achieve effective cytoreduction and reduce postoperative risks, improving early patient mobilization. Consequently, general anesthesia was administered to ensure optimal surgical conditions for laparoscopy.
In our patient, anesthetic management was meticulously tailored to the unique hemodynamic characteristics of Fontan physiology. The primary goals of our management were to maintain adequate preload, avoid increases in pulmonary vascular resistance, minimize intra-abdominal pressure, and preserve normal left ventricular afterload. Indeed, patients with Fontan circulation are highly sensitive to changes in intrathoracic pressure, preload, and afterload, any of which can precipitate hemodynamic decompensation because only the passive venous return drives pulmonary perfusion [3,5]. As a first-line approach, we opted for minimally invasive hemodynamic monitoring to guide fluid management. While intraoperative central venous pressure monitoring, reflecting Fontan circuit pressure, can assist in managing fluid therapy and identifying acute hemodynamic changes, we chose not to place a central venous catheter due to the increased risks of thrombosis and infective endocarditis. Likewise, transesophageal echocardiography has been reported to allow real-time intraoperative assessment of venous blood flow through the extracardiac Fontan circuit [11] and can be an appropriate option for hemodynamic monitoring in patients with Fontan circulation: intraoperative transesophageal echocardiography may provide useful information regarding the anatomy, function, and changes in conduit flow. In our case, a cardiologist was available to perform transesophageal echocardiography upon request in the event of hemodynamic instability or arrhythmias.
Anesthetic induction should prioritize hemodynamic stability. Agents such as etomidate or ketamine are often recommended owing to their minimal cardiovascular depressant effects. Although propofol is widely used, it should be administered cautiously and incrementally, as it can cause vasodilation and reduce preload [3,5]. In our case, propofol was titrated slowly under continuous hemodynamic monitoring.
Anesthesia maintenance can be safely achieved using low concentrations of volatile anesthetics in combination with intravenous agents such as opioids or dexmedetomidine [3,5]. Notably, volatile agents should be maintained at low minimum alveolar concentrations to avoid negative inotropy and systemic vasodilation. In our patient, general anesthesia was maintained with sevoflurane, in combination with sufentanil, titrated to achieve a minimum alveolar concentration between 1.0 and 1.5.
Ventilatory strategies should aim to minimize mean intrathoracic pressure, which can impair pulmonary blood flow in the absence of a subpulmonary ventricle. This includes the use of low tidal volumes, minimal or no positive end-expiratory pressure, and maintenance of normocapnia. Hypercapnia must be avoided, as elevated PaCO2 increases pulmonary vascular resistance and can further compromise pulmonary circulation. Various authors suggest that inspired oxygen should be titrated to maintain baseline or slightly elevated oxygen saturation, avoiding both hypoxia and hyperoxia [5].
Even though the pneumoperitoneum pressure had gradually risen to 12 mmHg, one of the most critical intraoperative phases was the creation of pneumoperitoneum, which decreased cardiac output and mean arterial pressure. Administration of a crystalloid bolus in our preload-dependent patient restored mean arterial pressure to the baseline value. Several authors describe the cumulative effect of increased intra-abdominal and intrathoracic pressure as producing significant hemodynamic compromise. Insufflation should be performed slowly, and intra-abdominal pressure should be maintained as low as possible, ideally below 10 to 12 mmHg, to reduce the risk of impaired venous return and increased intrathoracic pressure, both of which can sharply reduce cardiac output. For these reasons, continuous intraoperative hemodynamic monitoring is essential, and the surgical team must be prepared to convert to open surgery if hemodynamic instability ensues.
The SVV trend using the FloTrac system proved to be a useful tool in our case. It is noteworthy that the accuracy can be reduced in patients with low cardiac output states. Additionally, during laparoscopy, reliability may be compromised due to changes in intrathoracic and intra-abdominal pressures, as well as patient positioning. These factors can lead to false-positive or false-negative results when predicting fluid responsiveness using SVV. Wajima et al observed that SVV increased during pneumoperitoneum and decreased significantly afterward [13]. In any case, SVV can be an adequate dynamic indicator of fluid responsiveness during laparoscopic procedures [14,15]. We used SVV in conjunction with other clinical data and considered alternative dynamic tests, such as the fluid challenge, when necessary, to guide the fluid regimen.
Vasoactive agents can be required to support systemic perfusion. We had a dilute norepinephrine infusion prepared, as it can increase systemic vascular resistance and enhance myocardial contractility without significantly elevating pulmonary vascular resistance.
For patients who develop hypotension with low cardiac output, inodilators, such as milrinone, may be cautiously considered owing to their lusitropic and inotropic benefits. However, their vasodilatory effects necessitate careful titration and close hemodynamic monitoring.
In cases of laparotomic surgery, regional anesthesia, such as combined spinal-epidural, has been reported as a suitable anesthetic option for patients with univentricular circulation [16]. The advantages of regional anesthesia in this population are primarily related to the preservation of spontaneous ventilation, which facilitates pulmonary blood flow through the generation of negative intrathoracic pressure during inspiration. It is important to note that although neuraxial anesthesia has the intrinsic benefit of preserving preload in patients with single-ventricle physiology, it must be administered with caution because of the risk of sympathetic blockade, which can significantly decrease systemic vascular resistance and venous return [17].
Nonetheless, adjunctive regional techniques, such as abdominal wall blocks, can provide effective, opioid-sparing postoperative analgesia for abdominal procedures. In our patient, no regional block was performed, because of the minimally invasive nature of the laparoscopic approach.
In the immediate postoperative period, several authors recommend paying attention to fluid balance, oxygenation, ventilation, and analgesia. Postoperatively, as during the intraoperative period, hypovolemia, hypoxia, hypercapnia, and sympathetic activation due to poorly controlled pain can all worsen hemodynamic status and should be proactively managed [3,4].
Conclusions
In summary, anesthetic management of patients with Fontan physiology undergoing laparoscopy requires strategies to preserve preload, avoid elevated pulmonary vascular resistance, and minimize intrathoracic and intra-abdominal pressures. This case highlights the importance of minimally invasive hemodynamic monitoring to guide anesthetic management in patients with Fontan repair undergoing laparoscopy.
Figures
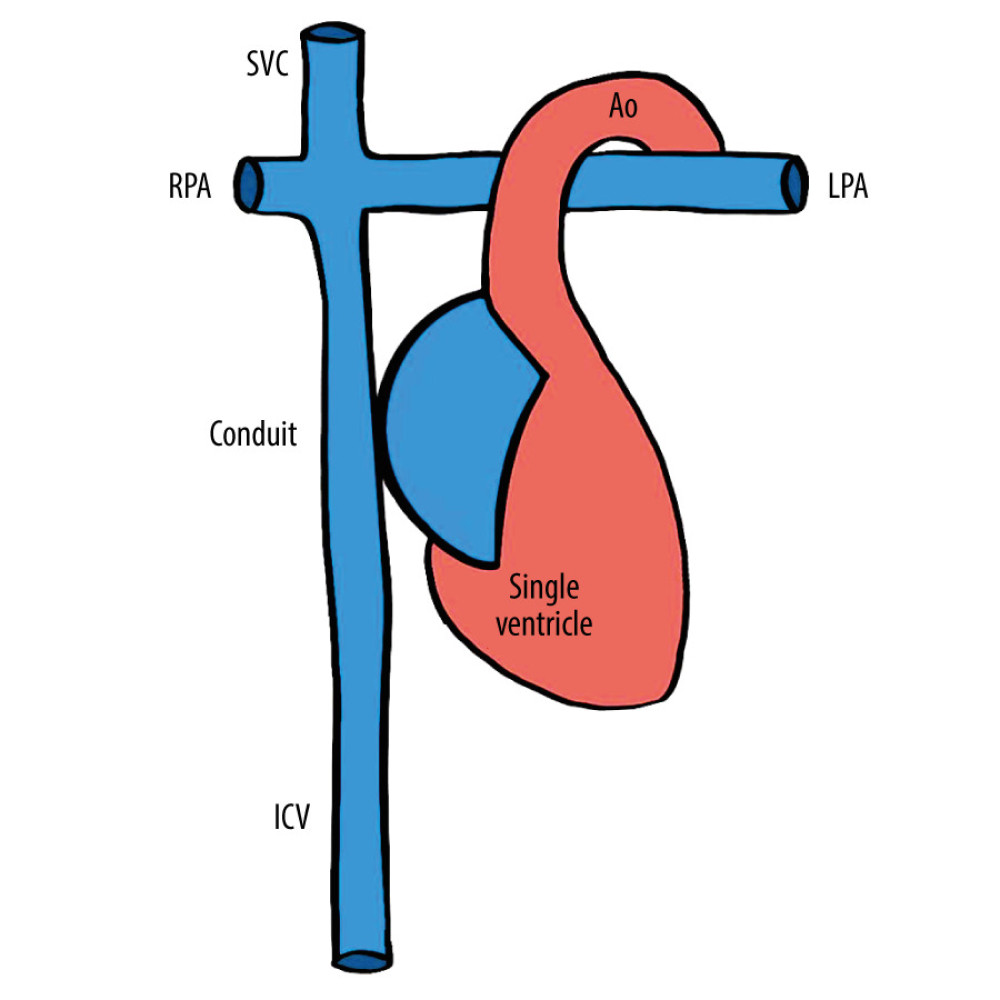 Figure 1. Schematic representation of the patient’s Fontan circulation. SVC – superior vena cava; IVC – inferior vena cava; RPA – right pulmonary artery; LPA – left pulmonary artery; Ao – aorta.
Figure 1. Schematic representation of the patient’s Fontan circulation. SVC – superior vena cava; IVC – inferior vena cava; RPA – right pulmonary artery; LPA – left pulmonary artery; Ao – aorta. 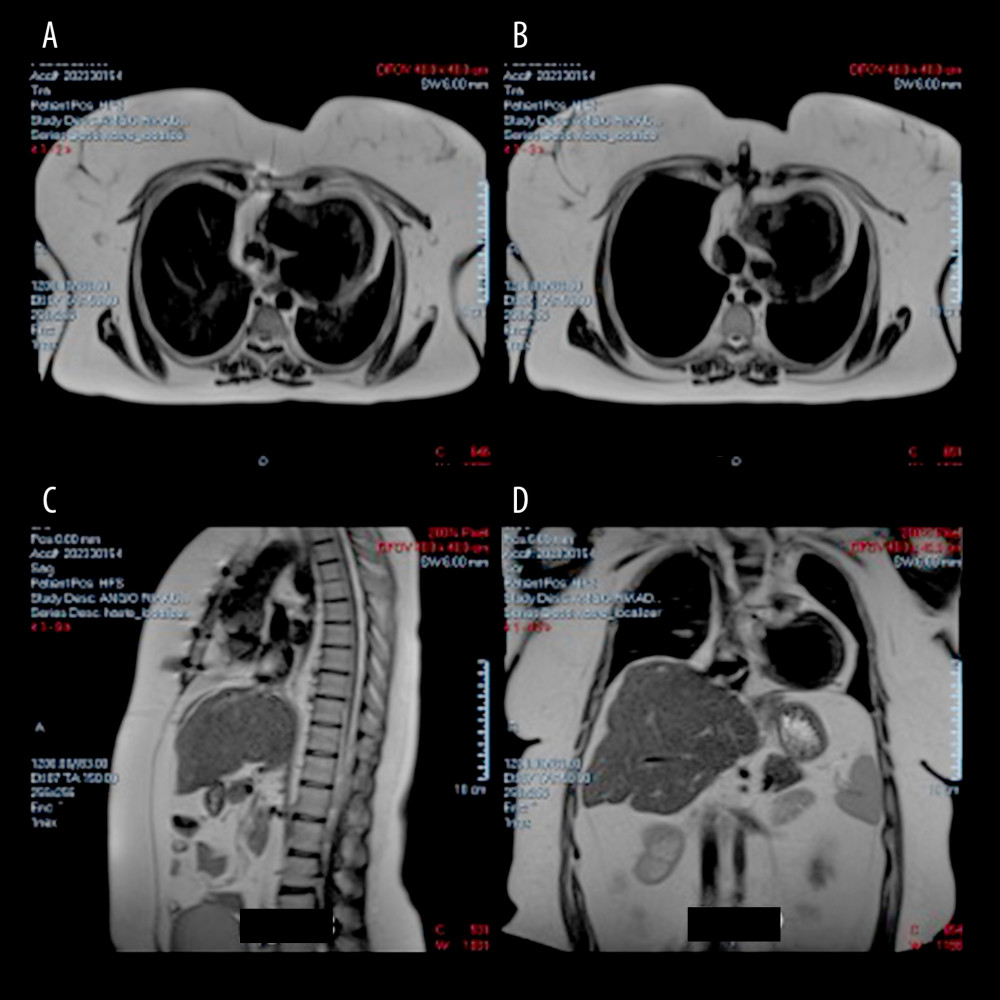 Figure 2. (A, B) Axial magnetic resonance imaging (MRI) scans showing the patient’s single ventricle after Fontan surgery. (C) Sagittal MRI scan showing the patient’s single ventricle after Fontan surgery. (D) Coronal MRI scan showing the patient’s single ventricle after Fontan surgery.
Figure 2. (A, B) Axial magnetic resonance imaging (MRI) scans showing the patient’s single ventricle after Fontan surgery. (C) Sagittal MRI scan showing the patient’s single ventricle after Fontan surgery. (D) Coronal MRI scan showing the patient’s single ventricle after Fontan surgery. 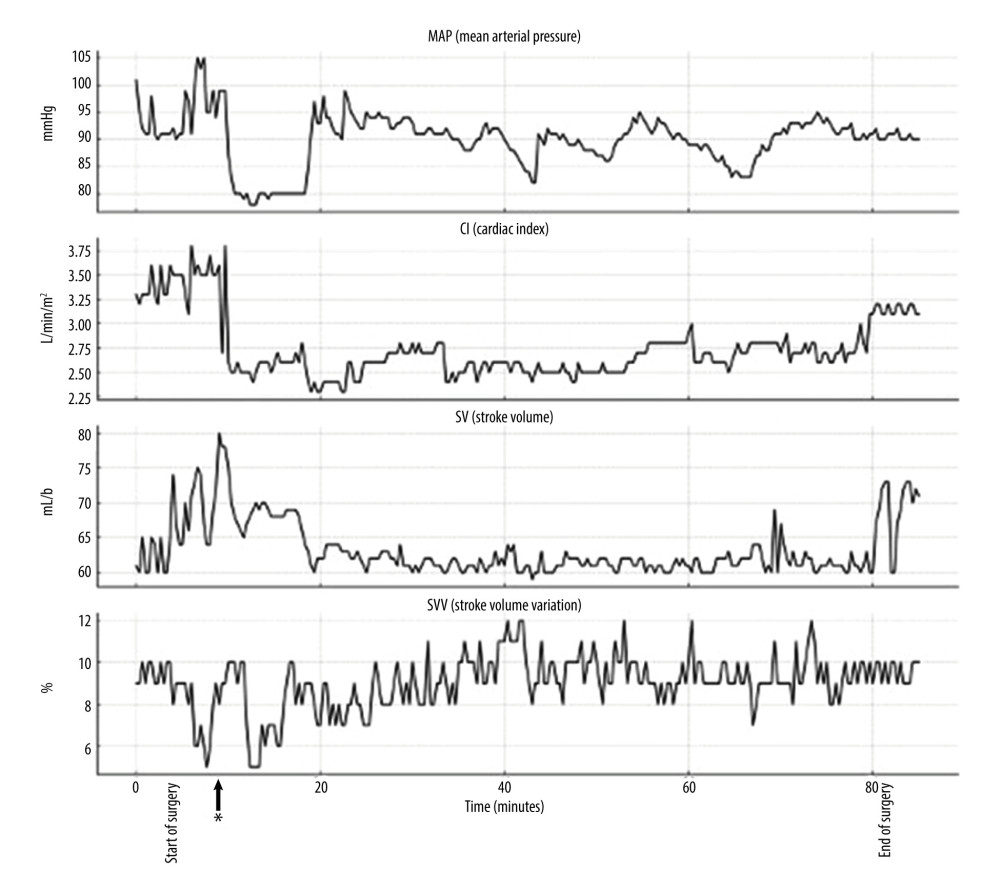 Figure 3. Hemodynamic parameters recorded during laparoscopy. * Start of pneumoperitoneum.
Figure 3. Hemodynamic parameters recorded during laparoscopy. * Start of pneumoperitoneum. 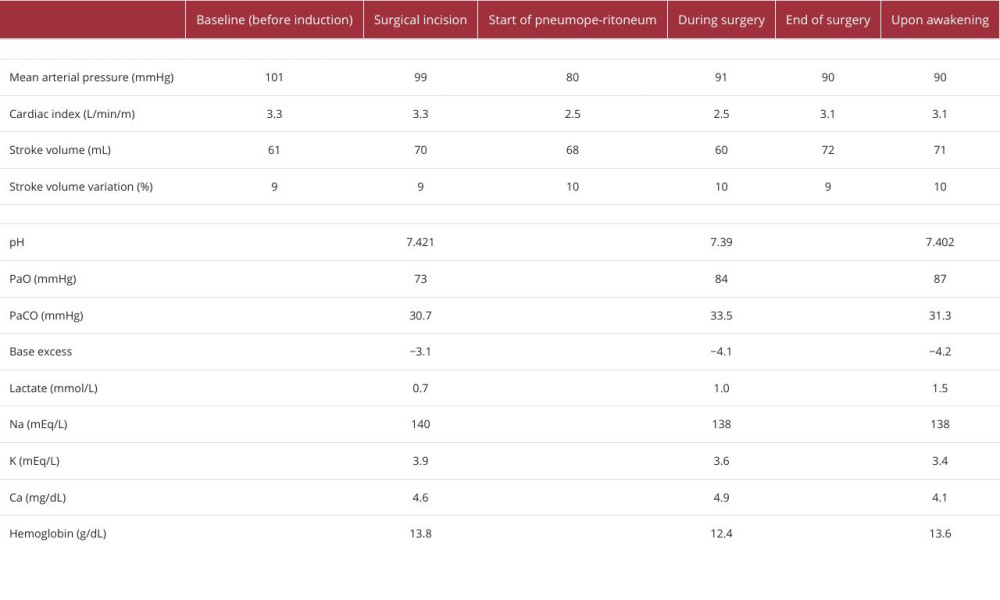
References
1. Khairy P, Poirier N, Mercier LA, Univentricular heart: Circulation, 2007; 115(6); 800-812
2. Lee M, Alahmadi MH, Shahjehan RD, Fontan completion: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing
3. Yuki K, Casta A, Uezono S, Anesthetic management of noncardiac surgery for patients with single ventricle physiology: J Anesth, 2011; 25(2); 247-56
4. McCandless RT, Bryner B, Perioperative management of the adult Fontan patient: Curr Opin Anaesthesiol, 2017; 30(3); 402-8
5. Neethling E, Heggie JE, Considerations in critical-care and anesthetic management of adult patients living with Fontan circulation: Can J Cardiol, 2022; 38(7); 1100-10
6. Takemoto S, Asada M, Maki J, Anesthetic management of an adult patient post a Fontan procedure in laparoscopic surgery: A case report: Cureus, 2024; 16(5); e59594
7. Dell’Anna AM, Grieco DL, Russo A, Case scenario: Perioperative management of a young woman with Fontan repair for major gynecologic surgery: Anesthesiology, 2016; 124(2); 464-70
8. Zach KJ, Ramakrishna H, Chandrasekaran K, Weis RA, Laparoscopic colectomy in an adult with single ventricle physiology: Anesthetic implications and management: Ann Card Anaesth, 2015; 18(2); 252-56
9. Saito K, Toyama H, Saito M, Yamauchi M, Successive perioperative management of laparoscopic liver resection in the reverse Trendelenburg position for a patient with Fontan physiology: A case report: JA Clin Rep, 2021; 7(1); 56
10. Kikuchi K, Iura A, Hara N, Anesthetic management during laparoscopic liver resection in a patient with Fontan physiology and high central venous pressure: J Cardiothorac Vasc Anesth, 2024; 38(8); 1742-45
11. Tankul R, Rodrigues B, Duggan LV, Laparoscopic cholecystectomy in a patient with Fontan circulation: Can J Anaesth, 2024; 71(10); 1417-22
12. Pundi KN, Pundi KN, Kamath PS, Liver disease after Fontan operation: Screening, management, and transplant considerations: Circulation, 2017; 136(15); 1323-34
13. Wajima Z, Shiga T, Imanaga K, Pneumoperitoneum affects stroke volume variation in humans: J Anesth, 2015; 29(4); 508-14
14. Zhang Z, Lu B, Sheng X, Jin N, Accuracy of stroke volume variation in predicting fluid responsiveness: A systematic review and meta-analysis: J Anesth, 2011; 25(6); 904-16
15. Messina A, Caporale M, Calabrò L, Reliability of pulse pressure and stroke volume variation in assessing fluid responsiveness in the operating room: A metanalysis and a metaregression: Crit Care, 2023; 27(1); 431
16. Catarci S, Sbaraglia F, Zanfini BA, Combined spinal-epidural anesthesia for urgent cesarean section in a parturient with a single ventricle: A case report: Korean J Anesthesiol, 2016; 69(6); 632-34
17. Ingram DA, Girling LG, Freed DH, Neuraxial blockade in patients with single-ventricle physiology: A word of caution: Anesth Analg, 2004; 99(1); 261-63
Figures
Figure 1. Schematic representation of the patient’s Fontan circulation. SVC – superior vena cava; IVC – inferior vena cava; RPA – right pulmonary artery; LPA – left pulmonary artery; Ao – aorta.Figure 2. (A, B) Axial magnetic resonance imaging (MRI) scans showing the patient’s single ventricle after Fontan surgery. (C) Sagittal MRI scan showing the patient’s single ventricle after Fontan surgery. (D) Coronal MRI scan showing the patient’s single ventricle after Fontan surgery.Figure 3. Hemodynamic parameters recorded during laparoscopy. * Start of pneumoperitoneum. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133