19 December 2025: Articles 
Concomitant Neurosarcoidosis and Cardiac Sarcoidosis: A Peculiar Path to Diagnosis
Unusual clinical course, Challenging differential diagnosis, Rare coexistence of disease or pathology
Meghan Stevenson EF 1*, Naveed Younis E 2DOI: 10.12659/AJCR.950208
Am J Case Rep 2025; 26:e950208






Abstract
BACKGROUND: Sarcoidosis is a multisystem inflammatory disorder characterized by non-caseating granulomas. Although the disease most commonly affects the respiratory and lymphatic systems, extrapulmonary manifestations involving the brain and heart also occur. Neurosarcoidosis may cause dysfunction of the cranial nerves, meninges, peripheral nerves, or the pituitary system. Cardiac sarcoidosis may lead to arrhythmias, cardiomyopathy, or heart failure. These specific diagnoses can be challenging because they may masquerade as isolated pathologies. In this clinical vignette, we present a rare case of systemic sarcoidosis with concomitant neurological and cardiac involvement.
CASE REPORT: A woman in her late 50s with a history of bilateral anterior uveitis presented with stroke-like symptoms. Initial workup was negative for stroke, but imaging identified a prevascular mediastinal lymph node and moderate mitral regurgitation. Lumbar puncture results were consistent with neurosarcoidosis, and steroids initiation led to symptom improvement. The patient subsequently exhibited non-sustained ventricular tachycardia, and further investigation revealed findings consistent with cardiac sarcoidosis. An implantable cardioverter-defibrillator was placed. The patient continued steroids and immunosuppressive therapy with favorable results.
CONCLUSIONS: Diagnosis of systemic sarcoidosis can be difficult because of its variable presentation. This challenge is enhanced when uncommon organs such as the brain and heart are affected. Thorough evaluation is therefore essential when evaluating systemic diseases.
Keywords: Cardiology, Neurology, sarcoidosis, Humans, Female, Central Nervous System Diseases, Cardiomyopathies, Middle Aged, Diagnosis, Differential
Introduction
Sarcoidosis is a multisystem disease that most commonly affects the lymphatic and pulmonary systems, although organs such as the heart and brain may also be involved. Diagnosis of extrapulmonary disease is challenging because symptoms are often nonspecific and mimic other conditions, which may result in prolonged evaluation, delayed treatment, and worse outcomes [1]. To aid this diagnostic process, widely accepted criteria classify neurosarcoidosis and cardiac sarcoidosis as possible, probable, or definite. This case highlights the diagnostic pathway when initial presentation mimics stroke despite normal angiotensin-converting enzyme (ACE) levels.
Case Report
A woman in her late 50s presented with facial droop, aphasia, and headache. She had a history of bilateral anterior uveitis and no clinically significant prior neurological or cardiac disease. Associated symptoms included nausea, neck pain, blurry vision, and hand paresthesia. Stroke workup was completed on the day of admission, beginning with head computed tomography (CT), which showed no intracranial hemorrhage or infarct. Head magnetic resonance imaging (MRI) with and without contrast showed no mass, edema, hydrocephalus, shift, or restricted diffusion. Carotid Doppler ultrasound showed no clinically significant stenosis. An electrocardiogram obtained on the day of admission showed a new right bundle branch block with ST abnormalities in inferior leads (Figure 1). A transthoracic echocardiogram completed on day 2 revealed moderate mitral regurgitation, biatrial enlargement, and a preserved ejection fraction of 50%; no interatrial shunt was identified. The patient’s headache and dysarthria recurred on day 3, prompting an infectious workup including a lumbar puncture due to suspicion of meningitis, as well as head and neck CT angiography for further assessment. Cerebrospinal fluid (CSF) analysis showed lymphocytic pleocytosis with 0.055×109/L total nucleated cells, 8% neutrophils, 5.9 mmol/L glucose, 1.61 g/L total protein, 871 mg/L albumin, and 100 mg/L IgG. The IgG synthesis rate was 8.53 mg/day. CSF tests showed negative results for infectious sources including
Head and neck CT angiography showed no focal stenosis, aneurysm, or large-vessel occlusion; it partially visualized a prevascular lymph node in the anterior mediastinum. Dedicated CT of the chest, abdomen, and pelvis was completed on day 4, confirming a 0.9 cm prevascular lymph node. Given the CSF results, history of bilateral anterior uveitis, prevascular mediastinal lymph nodes, and exclusion of alternative diagnoses, aseptic meningitis secondary to neurosarcoidosis was suspected. Based on guidance from the Neurosarcoidosis Consortium Consensus Group, the patient met criteria for possible neurosarcoidosis due to positive clinical presentation and supportive CSF findings. ACE was measured to potentially provide further diagnostic support, but the level was within normal limits. The patient began intravenous dexamethasone 4 mg every 6 h and showed considerable symptom improvement.
On day 5, the patient developed pulmonary edema. Repeat transthoracic echocardiography showed a stable ejection fraction of 50% with moderate to severe mitral regurgitation and elevated pulmonary artery systolic pressure (50–55 mmHg; Figure 2). The patient was transitioned from dexamethasone to intravenous methylprednisolone 250 mg every 6 h for 2 days, followed by prednisone 40 mg daily, which was tapered. On day 9, the patient exhibited a 21-beat run of non-sustained ventricular tachycardia (Figure 3). She subsequently underwent right and left heart catheterization procedures, which showed severe mitral regurgitation and no obstructive coronary artery disease. The patient was then cleared for discharge with plans for cardiac MRI and close electrophysiology follow-up. Cardiac MRI was completed on day 23 due to suspicion of cardiac sarcoidosis. This examination identified extensive mid-myocardial and epicardial non-ischemic enhancement, as well as apical wall thinning (Figure 4). The left ventricular ejection fraction was 46%, and dyssynchronous contractility was evident. The greatest involvement of the left ventricle occurred in the inferior wall, which demonstrated mural thinning most pronounced at the basilar and mid segments. This region was hypokinetic compared with the remaining left ventricle.
The patient returned with complaints of dizziness and palpitations; she was readmitted to the hospital. Given her recent history of non-sustained ventricular tachycardia and extensive cardiac scarring, she was considered high-risk for sudden cardiac death, which prompted placement of a biventricular implantable cardioverter-defibrillator (ICD). She also began oral amiodarone 100 mg daily, and a MitraClip was placed to treat mitral regurgitation. The patient tolerated the procedures with full neurological recovery and was discharged. Approximately 1 month later, she began infliximab infusion with oral methotrexate 15 mg and folic acid 1 mg. She then underwent a myocardial perfusion and metabolism positron emission tomography/computed tomography (PET/CT) scan for further evaluation of cardiac sarcoidosis. The scan showed mild fluorodeoxyglucose (FDG) uptake involving the anterior, septal, inferior, and inferolateral walls, as well as the basal inferoseptum, inferior, and inferolateral walls. The standardized uptake value was not reported; thus, tissue metabolic activity was not determined. Neither perfusion-metabolism mismatch nor suppression adequacy was addressed. FDG uptake in mediastinal lymph nodes and hyperintensity in the third thoracic vertebra were noted, indicative of a benign bone island. Endomyocardial biopsy was not performed due to low diagnostic accuracy – lesions are often missed because of patchy disease distribution. The patient developed respiratory failure 1 week later, prompting readmission to the hospital. This event was attributed to the infliximab infusion; therefore, both infliximab and methotrexate were paused until she recovered from the acute illness. Approximately 2 weeks later, she was transitioned to adalimumab 40 mg subcutaneously every 2 weeks with resumption of methotrexate. These medications were tolerated adequately.
According to the diagnostic criteria discussed below, the patient met qualifications for probable cardiac sarcoidosis based on cardiac MRI and FDG-PET findings, in addition to arrhythmogenic disease. No histological confirmation was conducted because biopsy was not considered necessary. She continued electrophysiology follow-up for arrhythmia management. Device interrogation of the biventricular ICD nearly 7 months later – approximately 10 months after initial presentation – showed a biventricular paced rhythm 86% of the time with premature ventricular contractions and sinus tachycardia. Amiodarone was then discontinued. Methotrexate was also discontinued, and mycophenolate mofetil was initiated at 1 g twice daily. Four months later, the patient underwent repeat FDG PET/CT, which showed decreased perfusion along the mid to basal inferior and inferolateral walls on resting PET perfusion images. Cardiac FDG images demonstrated interval resolution of FDG activity within the mid to basal inferior and inferolateral walls relative to imaging from 1 year prior. No new areas of FDG activity were identified in the myocardium. Extracardiac FDG findings included abnormal uptake at the gastroesophageal junction with a maximum standardized uptake value of 5.59 and uptake in the bilateral hilar lymph nodes. Based on these findings, there was no evidence of active cardiac sarcoidosis at that time. The patient reported occasional palpitations, which were identified as non-sustained ventricular tachycardia likely secondary to scarring. She reported no other symptoms.
Discussion
The course of this patient’s disease was complex and non-linear, requiring exclusion of several other diseases before a final diagnosis could be reached. The patient initially presented with features suggestive of stroke; extensive multimodal diagnostic testing ultimately led to the diagnosis of possible neurosarcoidosis and probable cardiac sarcoidosis, even in the setting of normal ACE levels. Although this putative diagnosis may not appear ground-breaking because it was not definitive, the patient tolerated the treatment regimen well and demonstrated substantial clinical improvement, further supporting the diagnosis. Despite this early favorable outcome, long-term follow-up is required to assess treatment success. The present follow-up is especially important because the present case reflects a single patient’s experience.
The Neurosarcoidosis Consortium Consensus Group developed diagnostic criteria for neurosarcoidosis that categorize patients into 3 groups: possible, probable, and definite. Possible neurosarcoidosis includes a positive clinical presentation with diagnostic evaluation – such as MRI, CSF analysis, or electromyography/nerve conduction studies – suggesting granulomatous inflammation of the nervous system. The patient in the present case met criteria for possible neurosarcoidosis through CSF findings and a positive clinical presentation. Probable neurosarcoidosis requires these findings in addition to pathological confirmation of systemic granulomatous disease. Definite neurosarcoidosis includes the prior criteria, as well as nervous system pathology consistent with neurosarcoidosis [2]. Serum ACE levels may be elevated in 30% to 80% of individuals with active sarcoidosis and can help monitor treatment response because granulomas produce ACE. However, ACE levels are not always elevated, as demonstrated in the presence case [3].
Although no randomized, double-blind, placebo-controlled treatment trials currently exist for neurosarcoidosis, it is accepted that patients should initially receive steroids such as prednisone [4]. Treatment is continued in a stepwise manner. For severe disease or progression despite oral therapy, methylprednisolone is typically used. Our patient began with dexamethasone but required escalation to methylprednisolone followed by a prednisone taper. If steroids are ineffective, second-line treatment includes steroid-sparing agents such as methotrexate, mycophenolate, azathioprine, or leflunomide. Methotrexate is most widely used, though other agents may be selected according to toxicity profiles. Tumor necrosis factor inhibitors (eg, infliximab) constitute the next preferred option. Given the severe brain and heart involvement in our patient, infliximab infusion with methotrexate was recommended. She did not tolerate infliximab and was transitioned to adalimumab, which is recommended in such cases. Intravenous cyclophosphamide has also been used in refractory disease, and rituximab is reportedly useful when tumor necrosis factor-alpha inhibitors are contraindicated [5]. Fortunately, our patient tolerated adalimumab well and required no additional regimen.
There are 2 generally accepted pathways for diagnosis of cardiac sarcoidosis. The first requires histological confirmation of noncaseating granulomas through endomyocardial biopsy, left ventricular core biopsy, or examination of explanted hearts. Because infiltration in this disease is often patchy, the overall sensitivity of endomyocardial biopsy is low; lesions may be missed. To address this limitation, cardiac sarcoidosis can also be diagnosed through a combination of clinical, pathological, and imaging modalities. Using these criteria, definite diagnosis requires detection of noncaseating granulomas on histology with no alternative etiology identified. Highly probable cardiac sarcoidosis requires confirmed diagnosis of extracardiac sarcoidosis, clinical findings consistent with cardiac sarcoidosis, and imaging findings consistent with cardiac sarcoidosis as identified by cardiac MRI or FDG-PET. Other possible etiologies must be excluded. Cardiac MRI is particularly useful because it identifies both inflammation and scarring, whereas FDG-PET assesses only inflammation. These modalities can support a diagnosis of sarcoidosis even when ACE levels are normal. If histological evidence of extracardiac sarcoidosis is present, the diagnosis of probable cardiac sarcoidosis can be made when clinical and imaging findings are consistent with cardiac sarcoidosis. If there is no histological or clinical diagnosis of extracardiac sarcoidosis, diagnostic criteria require imaging findings on both cardiac MRI and FDG-PET, as well as at least 1 clinical feature consistent with cardiac sarcoidosis. Other potential causes must again be excluded. Although the present case did not include histological confirmation, the patient demonstrated compelling imaging findings and a new arrhythmia, which constituted a clinical feature. Possible or low-probability cardiac sarcoidosis includes patients who do not meet criteria for definite, highly probable, or probable cardiac sarcoidosis. Similar to neurosarcoidosis, cardiac sarcoidosis is typically treated with first-line steroids, followed by immunosuppressive agents. Although ICD implantation is generally reserved for secondary prevention of sudden cardiac death, it is reasonable in patients with an ejection fraction greater than 35% when myocardial scarring is identified on cardiac MRI or FDG-PET, given the increased risk of sudden cardiac death [6].
Neurological involvement occurs in approximately 5% to 10% of patients diagnosed with sarcoidosis, and cardiac involvement occurs in 5% to 30% of patients. The increased prevalence of cardiac sarcoidosis is largely attributed to advancements in cardiac imaging [7,8]. A single-institution retrospective cohort study showed that 12% of patients diagnosed with neurosarcoidosis eventually developed cardiac sarcoidosis, suggesting that patients with neurological involvement should be evaluated for concomitant cardiovascular disease [9]. Early recognition can improve overall outcomes by preventing arrhythmias and cardiomyopathies. This prevention is particularly important because cardiac sarcoidosis often goes undiagnosed antemortem due to the high incidence of sudden cardiac death [1]. Research has not yet clarified whether an underlying process links these 2 diseases; future studies may focus on establishing such a connection. Although arrhythmias are a common manifestation of cardiac sarcoidosis, valve involvement is not. It is also unusual for a patient to be diagnosed simultaneously with both neurosarcoidosis and cardiac sarcoidosis, making the present case especially notable.
Conclusions
This case illustrates how the integration of brain and CSF evaluation with cardiac MRI and FDG-PET can support a working diagnosis of concomitant neurosarcoidosis and cardiac sarcoidosis despite a normal ACE level. Early corticosteroid therapy and timely ICD placement are imperative to address both inflammatory activity and arrhythmia risk.
Figures
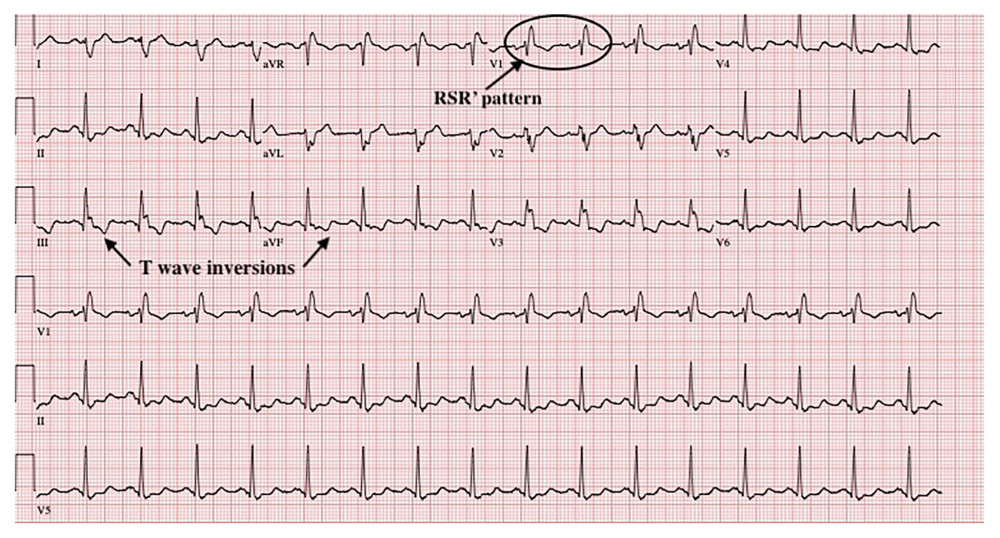 Figure 1. Echocardiogram illustrating a right bundle branch block with ST abnormalities in inferior leads.
Figure 1. Echocardiogram illustrating a right bundle branch block with ST abnormalities in inferior leads. 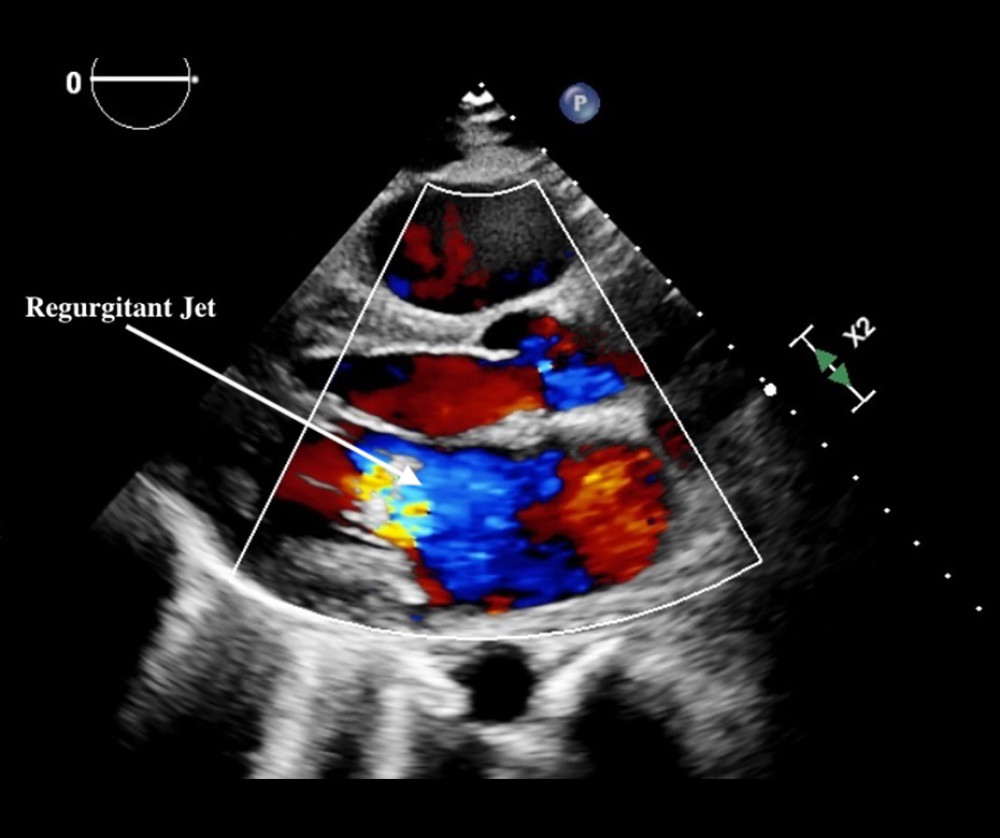 Figure 2. Color flow Doppler transthoracic echocardiogram showing mitral regurgitation in the parasternal long-axis view.
Figure 2. Color flow Doppler transthoracic echocardiogram showing mitral regurgitation in the parasternal long-axis view. 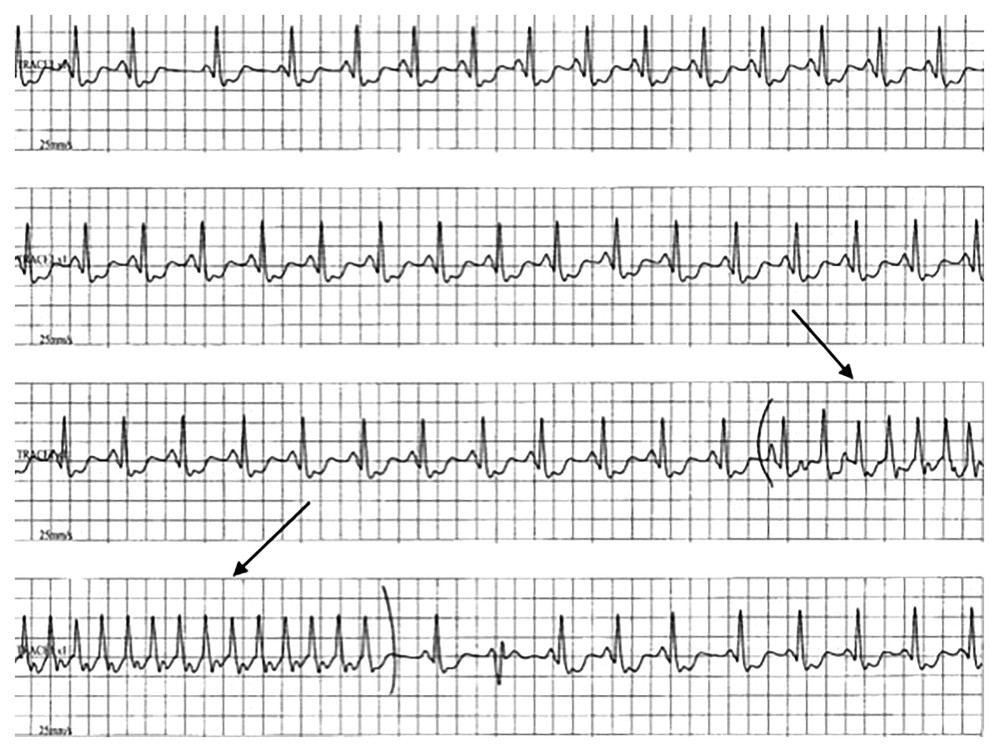 Figure 3. Echocardiogram illustrating progression to a 21-beat run of non-sustained ventricular tachycardia.
Figure 3. Echocardiogram illustrating progression to a 21-beat run of non-sustained ventricular tachycardia. 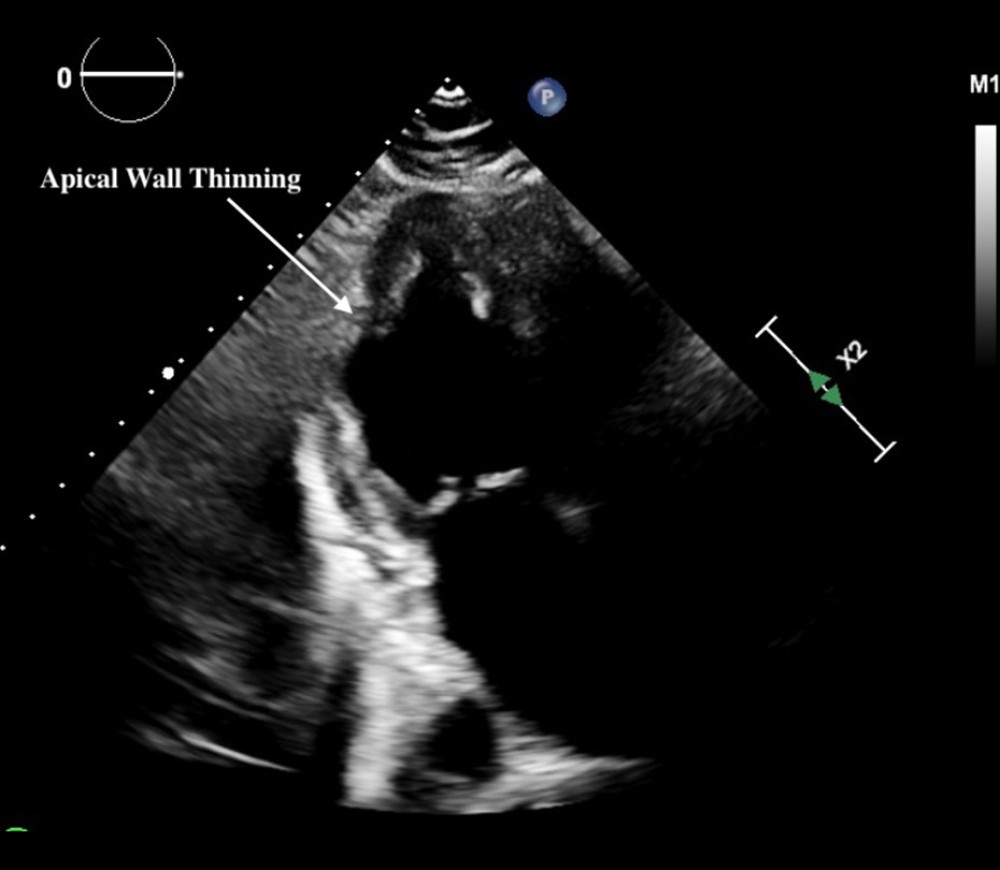 Figure 4. Late gadolinium enhancement cardiac magnetic resonance imaging scan showing apical wall thinning secondary to inflammation from sarcoidosis.
Figure 4. Late gadolinium enhancement cardiac magnetic resonance imaging scan showing apical wall thinning secondary to inflammation from sarcoidosis. References
1. Belperio JA, Shaikh F, Abtin F, Extrapulmonary sarcoidosis with a focus on cardiac, nervous system, and ocular involvement: EClinicalMedicine, 2021; 37; 100966
2. Bradshaw MJ, Pawate S, Koth LL, Neurosarcoidosis: Neurol Neuroimmunol Neuroinflamm, 2021; 8(6); e1084
3. Zheng S, Du X, Dong J, Re-evaluating serum angiotensin-converting enzyme in sarcoidosis: Front Immunol, 2023; 14; 950095
4. Stern BJ, Corbett J, Neuro-ophthalmologic manifestations of sarcoidosis: Curr Treat Options Neurol, 2007; 9(1); 63-71
5. Voortman M, Drent M, Baughman RP, Management of neurosarcoidosis: A clinical challenge: Curr Opin Neurol, 2019; 32(3); 475-83
6. Cheng RK, Kittleson MM, Beavers CJ, Diagnosis and management of cardiac sarcoidosis: A scientific statement from the American Heart Association: Circulation, 2024; 149(21); e1197-216
7. Pirau L, Lui F, Neurosarcoidosis: StatPearls [Internet], 2020, Treasure Island (FL), StatPearls Publishing Available from:https://www.ncbi.nlm.nih.gov/books/NBK534768/
8. Ribeiro Neto ML, Jellis CL, Joyce E, Update in cardiac sarcoidosis: Ann Am Thorac Soc, 2019; 16(11); 1341-50
9. Noroozi Gilandehi S, Wong KH, Francis T, Cardiac involvement in neurosarcoidosis: A single-center investigation: Neurol Neuroimmunol Neuroinflamm, 2024; 11(2); e200196
Figures
Figure 1. Echocardiogram illustrating a right bundle branch block with ST abnormalities in inferior leads.Figure 2. Color flow Doppler transthoracic echocardiogram showing mitral regurgitation in the parasternal long-axis view.Figure 3. Echocardiogram illustrating progression to a 21-beat run of non-sustained ventricular tachycardia.Figure 4. Late gadolinium enhancement cardiac magnetic resonance imaging scan showing apical wall thinning secondary to inflammation from sarcoidosis. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133