24 December 2025: Articles 
Conception After Chemotherapy for Intraplacental Choriocarcinoma: Favorable 5-Year Follow-Up of the Mother and Child
Rare disease
Tomoo Suzuki ABCDEF 1, Masanori OnoDOI: 10.12659/AJCR.950426
Am J Case Rep 2025; 26:e950426






Abstract
BACKGROUND: Intraplacental choriocarcinoma (IC) is a rare subtype of gestational choriocarcinoma that can be associated with placental hemorrhage and metastases to the mother and fetus. Chemotherapy can be effective in cases of placental localization and may not adversely affect fertility. This report describes a 32-year-old woman who conceived 10 months after chemotherapy for IC and achieved successful term delivery of that pregnancy.
CASE REPORT: A 32-year-old woman delivered her first child by vacuum extraction due to weak labor and fetal distress. The newborn presented with severe anemia, as well as elevated alpha-fetoprotein and fetal hemoglobin levels, suggesting fetomaternal hemorrhage. Placental histopathology revealed IC. Postpartum elevation of human chorionic gonadotropin levels prompted EMA-CO (etoposide, methotrexate, actinomycin D/cyclophosphamide, vincristine) chemotherapy; 7 treatment courses were completed without side effects or metastasis. Ten months after completion of chemotherapy, the patient spontaneously conceived. She subsequently delivered a healthy boy at 38+5 weeks of gestation; placental examination did not reveal malignancy. During the 5-year follow-up period, both children developed normally, and no maternal recurrence or metastasis was observed.
CONCLUSIONS: This report describes a case of postnatal diagnosis of IC via placental histopathology, followed by successful treatment and subsequent pregnancy within 1 year after chemotherapy completion. The findings highlight the importance of accurate diagnosis and appropriate management of IC; they support previous observations that chemotherapy does not preclude future successful pregnancies. Additionally, the report underscores the clinical challenges of IC, its implications for future pregnancies, and the need for long-term follow-up concerning both mother and child.
Keywords: Antineoplastic Combined Chemotherapy Protocols, Choriocarcinoma, Fetomaternal Transfusion, Follow-Up Studies, gestational trophoblastic disease, Pregnancy Outcome, Humans, Female, Pregnancy, adult, Uterine Neoplasms, Dactinomycin, Cyclophosphamide, Pregnancy Complications, Neoplastic, Vincristine, Methotrexate, Infant, Newborn, Etoposide, Male, Placenta
Introduction
Gestational trophoblastic disease (GTD) encompasses a heterogeneous group of pregnancy-related trophoblastic tumors, including hydatidiform mole, invasive mole, choriocarcinoma, and placental site and epithelioid trophoblastic tumors. GTD, typically involving abnormal uterine bleeding and elevated serum human chorionic gonadotropin (hCG) levels, is diagnosed based on quantitative hCG testing and histopathological findings; management follows International Federation of Gynecology and Obstetrics (FIGO) staging and World Health Organization risk scoring to guide chemotherapy selection [1]. Intraplacental choriocarcinoma (IC) is an extremely rare form, which represents approximately 0.04% of all GTD diagnoses [2,3]. IC, a choriocarcinoma confined to the placenta without metastasis, is often referred to as choriocarcinoma in situ [2]. Unlike typical choriocarcinoma, IC is usually asymptomatic, which hinders clinical diagnosis [4]. Although its pathogenesis remains unclear, IC can occur after any pregnancy, including normal pregnancies, hydatidiform moles, and miscarriages [5,6]. A notable challenge is that many cases have limited diagnostic opportunities due to the absence of maternal symptoms [7]. Approximately half of IC cases are incidentally diagnosed on placental histopathological examination after delivery [8]; additionally, these cases often involve microscopic lesions that are difficult to grossly distinguish from fresh infarcts or intervillous thrombi [9]. IC may lead to fetomaternal hemorrhage (FMH), which can result in fetal dysfunction or hemorrhage; IC diagnosis may also be prompted by fetal dysfunction or neonatal anemia [9]. However, few facilities routinely perform placental pathology, which further limits diagnostic opportunities [2].
There remain no standard guidelines for IC treatment; however, the treatment strategy is similar to that used for other types of gestational trophoblastic neoplasia (GTN) [10]. After removal of the tumor with the placenta, multiagent chemotherapy – typically etoposide + methotrexate + actinomycin D/cyclophosphamide + vincristine (EMA/CO) – is often selected based on blood hCG levels and the presence of metastases [11]. Tumors are highly sensitive to chemotherapy, and many patients achieve good outcomes [9]. Because treatment generally spares the uterus, fertility is relatively well preserved [12]. Nevertheless, the long-term prognosis of IC and its course after subsequent pregnancies remain unclear [13]. Further case reports are warranted to accumulate experience regarding the follow-up of patients with IC and management of subsequent pregnancies.
This report describes a 32-year-old woman who conceived 10 months after chemotherapy for IC and achieved successful term delivery of that pregnancy.
Case Report
The patient was a 32-year-old primipara with height 150 cm, weight 48 kg, and body mass index 21 kg/m2. Her menstrual cycle was regular, and she had no history of dysmenorrhea. The first pregnancy was spontaneous, and she received routine antenatal care without special interventions. During pregnancy, she did not experience excessive nausea or vomiting, and her uterine fundal height measurements were appropriate for gestational age. Ultrasonographic examination revealed no abnormalities; no significant anemia was observed before delivery.
At 39 weeks and 6 days of gestation, the patient underwent vacuum extraction at Kyorin University Suginami Hospital due to weak labor and fetal dysfunction. The baby was a girl weighing 2768 g. Her Apgar scores were 6 at 1 min, 6 at 5 min, and 6 at 10 min; her umbilical artery blood pH was 7.30, consistent with mild neonatal distress.
Immediately after birth, generalized pallor and prominent anemia (hemoglobin level: 3.4 g/dL; reference range for term neonates: 14–24 g/dL) were observed, requiring red blood cell transfusion; the baby was subsequently transferred to the neonatal intensive care unit. Blood tests on the day after delivery revealed elevated alpha-fetoprotein (9542 ng/mL; normal level: approximately 200 ng/mL at term) and fetal hemoglobin (4.5%; normal level: approximately 1% in maternal blood), strongly suggesting FMH. However, the patient did not undergo Kleihauer-Betke testing or flow cytometry. Given the observations of fetal dysfunction and suspected FMH, placental histopathological examination was performed immediately after delivery. Gross examination revealed a necrotic nest measuring approximately 4 cm in diameter extending from the basal plate to the fetal surface; the umbilical cord did not show abnormal findings (Figure 1). Histopathology (hematoxylin and eosin staining) revealed irregular proliferation of atypical trophoblasts and a mixture of mononuclear and multinuclear atypical cells, which are typical findings in placental choriocarcinoma (Figure 2). Magnetic resonance imaging and thoracoabdominal pelvic computed tomography did not reveal metastases.
At 2 months postpartum, the patient’s serum hCG levels were elevated again. Although metastases were not present, EMA/CO therapy was initiated because of the potential for metastatic disease. After 3 courses of chemotherapy, hCG negativity was confirmed. To prevent recurrence, 4 additional courses were administered. During treatment, blood tests did not reveal hepatic abnormalities, renal abnormalities, or bone marrow suppression, and hCG levels did not rise. No adverse effects were observed.
Ten months after completion of chemotherapy, the patient spontaneously conceived. For pregnancy management, transabdominal ultrasonography was performed every 4 weeks in the first trimester, every 2 weeks in the second trimester, and every 1 to 2 weeks in the third trimester; no abnormalities in placental position or fetal growth were identified. She was diagnosed with gestational diabetes mellitus, which remained well controlled with nutritional guidance and exercise therapy. There were no complications such as gestational hypertension, shortened cervical canal length, malignant genital bleeding, or fetal growth retardation.
At 38 weeks and 5 days of gestation, the second child was born via spontaneous vaginal delivery. The baby was a boy weighing 3168 g. His Apgar scores were 8 at 1 min and 9 at 5 min; his umbilical artery blood pH was 7.31. There was no recurrence of FMH at delivery, and the newborn did not require special treatment. Placental pathological examination revealed no abnormal findings, including no recurrence of placental choriocarcinoma, based on detailed evaluation of 18 placental sections. The mother also experienced no complications.
After delivery of the second child, follow-up examinations with blood hCG measurements were performed. Chest radiography was conducted at 3-month intervals; chest, abdominal, and pelvic computed tomography scans were performed annually. At the most recent assessment, 5 years had passed since completion of chemotherapy (3 years and 3 months after delivery of the second child). The mother and both children were in good physical and mental health, without evidence of recurrence or metastasis. Figure 3 shows hCG levels throughout the follow-up period.
Discussion
This case highlights the typical presentation, diagnostic pathway, and clinical course of IC, which is characterized by an asymptomatic maternal course, FMH-induced neonatal anemia, and definitive diagnosis via placental histopathology. These features are consistent with previously reported cases of IC, which have emphasized that the disease is often identified incidentally after delivery and that early pathological evaluation is essential for timely diagnosis and favorable outcomes [7–13].
This case also demonstrates the importance of early diagnosis and treatment of IC in achieving favorable maternal and neonatal outcomes. IC is a rare gestational trophoblastic tumor that occurs in approximately 1 in 50 000 normal pregnancies [14]. IC can result in FMH, fetal growth retardation, and stillbirth; moreover, the perinatal mortality rate of IC-related FMH is approximately 37% [9]. However, maternal prognosis is good with appropriate therapeutic intervention; the reported maternal mortality rate is approximately 5% [9]. This favorable prognosis is attributed to the high sensitivity of IC to chemotherapy, as well as the feasibility of uterus-sparing treatment [13].
Although reports of successful pregnancies after IC treatment remain limited, pregnancies and deliveries have been described approximately 1.5 to 3 years after completion of therapy. Sapantzoglou et al reported a case of successful pregnancy and delivery 18 months after treatment for metastatic choriocarcinoma that developed following a normal pregnancy and delivery [15]. Liu et al described a case of normal delivery 37 months after IC remission [13]. In both cases, there were no signs of recurrence in the mother, and the newborns were healthy; maternal and neonatal outcomes were favorable. Generally, GTN treatment is relatively fertility-preserving, without increased risk of subsequent pregnancy complications or fetal malformations, even among patients who receive multidrug chemotherapy [16]. Approximately 87% of women seeking conception after GTN treatment achieve pregnancy, and about 76% deliver healthy newborns at full term without adverse effects on pregnancy outcomes, regardless prior of multidrug chemotherapy [16]. FIGO guidelines indicate no need for pessimism concerning future pregnancies after GTN remission, noting that maternal and neonatal outcomes are favorable with appropriate treatment and follow-up [11]. This perspective is consistent with the present case, in which fertility was preserved and maternal and neonatal outcomes were favorable. Although guidelines recommend contraception for at least 1 year after remission, pregnancy occurred after 10 months in the present case. In contrast, Zhu et al analyzed 22 patients who conceived within 1 year after completing chemotherapy for GTN; they reported higher rates of fetal wastage (27.3%) and recurrent GTD (9.1%), supporting current recommendations to delay conception for at least 1 year after remission [17]. Nonetheless, no recurrence has been observed in our patient, consistent with more recent reports of favorable outcomes [13]. In the second pregnancy, the patient developed gestational diabetes mellitus. However, no published reports describe an association between IC and gestational diabetes mellitus, and previous reviews have not identified maternal metabolic disorders as risk factors for IC [2,9]. In the present case, the occurrence of gestational diabetes mellitus appeared incidental and unrelated to IC.
Given that IC is a subtype of choriocarcinoma, its treatment strategy is similar to that of other GTNs. In the present case, EMA/CO therapy was selected [11]. Multiagent chemotherapy (eg, EMA/CO) is recommended for the initial treatment of high-risk GTN in patients with a FIGO risk score of 7 or greater [11]. IC, a choriocarcinoma secondary to normal pregnancy, is considered to have a worse prognosis than complete hydatidiform moles. Because IC is often associated with invasion into the maternal circulation and potential metastasis [18], careful risk assessment is warranted even in the absence of clinically evident metastasis.
In the present case, extensive FMH was suspected at the time of delivery, and maternal hCG levels remained elevated after delivery, indicating a high risk of metastasis. Accordingly, EMA/CO therapy was initiated, comprising an effective regimen with a remission rate of 98% to 100% [19]. Complete remission was rapidly achieved. A prior report documented cases of patients with non-metastatic IC who underwent hCG monitoring without chemotherapy [2]. Duleba et al recommended strict post-treatment surveillance for non-metastatic IC and chemotherapy for metastatic IC, noting that some localized cases were successfully managed without therapy [20]. However, a literature review showed that approximately 2% of patients with non-metastatic IC subsequently experienced relapse with pulmonary metastases; thus, close follow-up is essential even for patients who do not receive chemotherapy [13]. Although our patient completely recovered after initial treatment, choriocarcinoma can aggressively invade the lungs, liver, or brain if latent metastases are missed and treatment is delayed. In such cases, the 5-year survival rate without treatment ranges from 20% to 40%, and the risk of poor prognosis is high without effective multiagent chemotherapy [21]. Overall, EMA/CO therapy was appropriate in the present case and constitutes a reasonable option to eradicate potential metastases.
Our patient’s IC has remained in remission, and her risk of recurrence is considered low. Approximately 96% of patients with non-metastatic IC reportedly do not experience recurrence [2], consistent with our findings. However, when malignant cells exhibit dissemination, close follow-up for a defined period after remission is essential. FIGO guidelines recommend follow-up with monthly hCG measurements for at least 12 months after treatment completion and avoidance of pregnancy during this period [11]. This approach allows early detection and treatment of any relapse, thereby supporting a favorable maternal prognosis.
Based on the above findings, future management policies should include: a) adequate follow-up with periodic hCG monitoring and imaging studies; b) strict contraceptive guidance during the follow-up period; and c) perinatal management in post-remission pregnancy cases, including exclusion of abnormal pregnancy via prompt ultrasonography, careful follow-up during pregnancy, close monitoring of the placenta after delivery, and confirmation of maternal hCG levels. Given sporadic reports of IC recurrence in the placenta [13], patients with a history of IC should undergo routine placental pathology examinations after delivery [22,23]. Psychological care should also be considered because some patients may abandon pregnancy plans after IC remission due to concerns about recurrence during future pregnancies [24,25]. Consistent long-term monitoring and comprehensive pregnancy care can help prevent recurrence and support safe delivery after IC remission.
Early diagnosis of IC is crucial. In our patient, prompt placental pathology after delivery enabled timely diagnosis. The incidence of IC associated with FMH remains unclear – only 29 cases have been reported since 1995 [9,14,26]. However, FMH may facilitate early IC diagnosis in utero through characteristic ultrasonographic findings during pregnancy. When fetal anemia or hydrops is suspected, detailed fetal ultrasonography is recommended to assess Doppler parameters (eg, middle cerebral artery velocity waveform) and overall fetal morphology [27,28].
As noted above, the number of reported IC cases remains limited. Case accumulation and centralized management through a rare cancer registry project should be considered. To our knowledge, this is the first report of pregnancy occurring within 1 year after treatment completion that did not involve recurrence in either the mother or child. Further case reports and studies are warranted. Although most patients with IC can achieve success via EMA/CO chemotherapy, new treatment strategies for refractory cases should be explored. Immune checkpoint inhibitors (eg, anti-programmed cell death protein 1 [PD-1]/programmed death-ligand 1 [PD-L1] antibodies) have shown effectiveness in patients with chemotherapy-refractory GTN; accordingly, evaluation of molecular targeted therapy and immunotherapy for IC is important [29]. Additionally, elucidation of the mechanisms underlying IC pathogenesis and identification of predictive factors for recurrence are needed. Although the genetic relationship between IC and the fetus/placenta has been examined [30], the genetic background of choriocarcinoma and its interaction with the placental microenvironment remain unclear.
Assessments of survival and quality of life after remission are also important. Notably, some patients with IC abandon future pregnancy plans because of anxiety regarding recurrence. Future studies should aim to improve psychosocial support systems and establish follow-up guidelines that allow patients to pursue pregnancy and childbirth with confidence.
Conclusions
This case report highlights the importance of placental histopathology in IC diagnosis and suggests that timely chemotherapeutic intervention is effective for maintaining long-term prognosis and fertility. It also demonstrates that favorable outcomes can be achieved with appropriate obstetric management, even when pregnancy occurs before the standard recommended contraceptive interval. This outcome is consistent with previous reports indicating that chemotherapy for GTD does not preclude future successful pregnancies. The practical perspectives demonstrated in this case – including thorough placental pathological evaluation, timely initiation of treatment, and careful perinatal management of post-remission pregnancy – may contribute to future standardization of clinical protocols regarding IC.
Figures
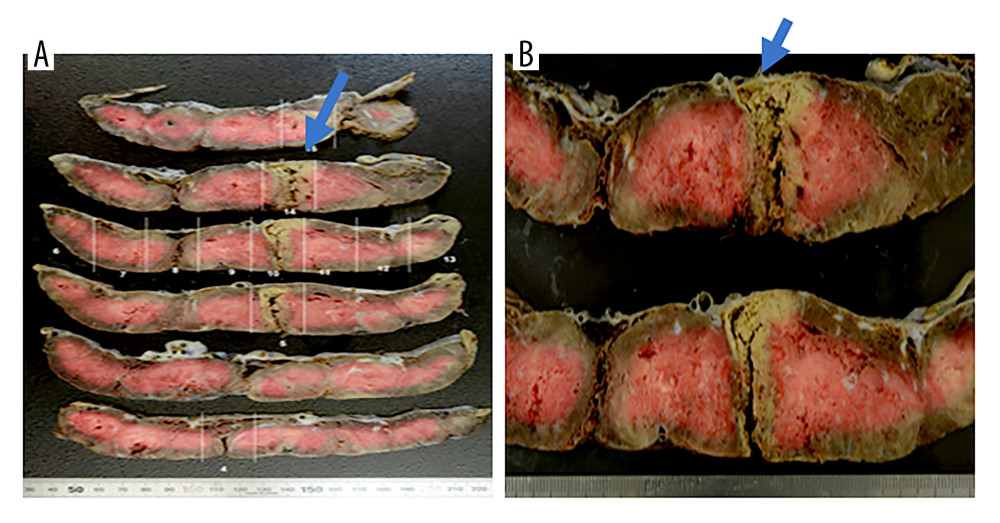 Figure 1. (A, B) Gross appearance of the placenta from the first pregnancy complicated by intraplacental choriocarcinoma. Gross examination of the placenta from the first pregnancy revealed a well-demarcated, brownish-white nodular lesion measuring 4 cm in diameter, with extensive areas of necrosis (arrows).
Figure 1. (A, B) Gross appearance of the placenta from the first pregnancy complicated by intraplacental choriocarcinoma. Gross examination of the placenta from the first pregnancy revealed a well-demarcated, brownish-white nodular lesion measuring 4 cm in diameter, with extensive areas of necrosis (arrows). 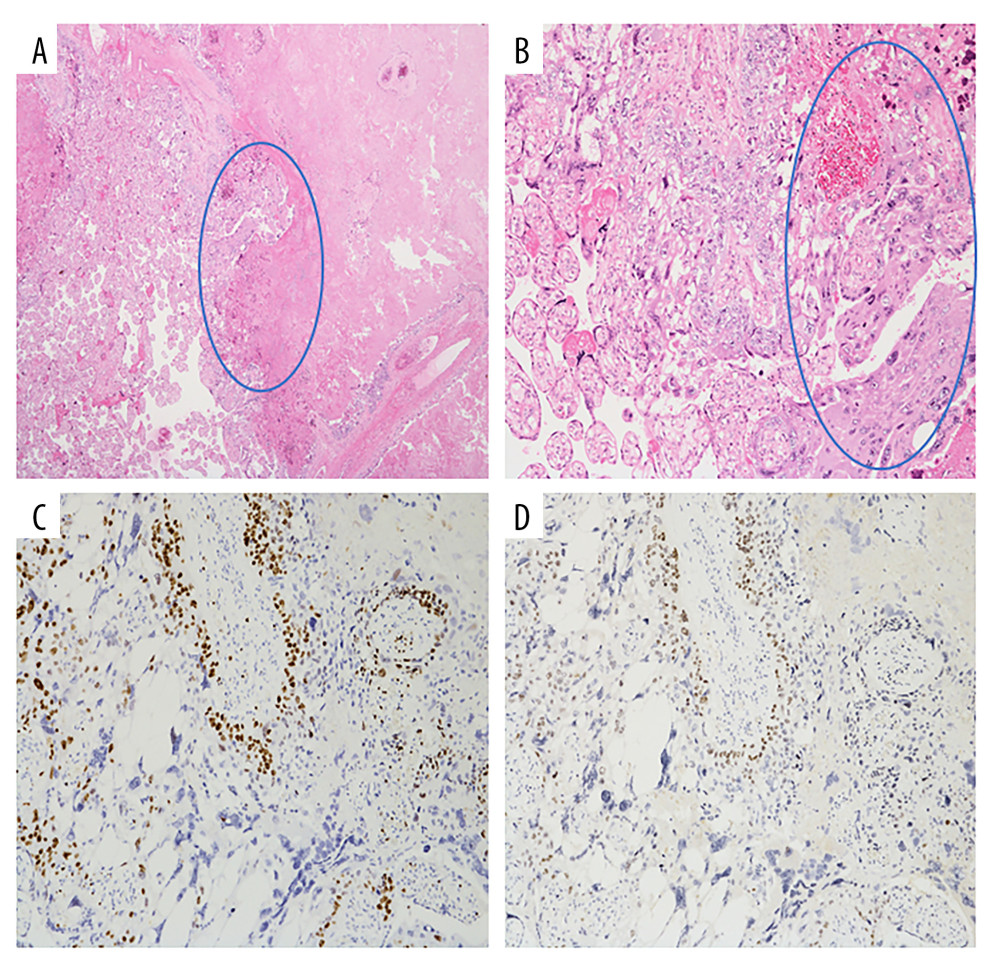 Figure 2. Histopathological findings of the placenta from the first pregnancy complicated by intraplacental choriocarcinoma(A) Hematoxylin and eosin (H&E) staining, ×20. The right side of the image shows a broad area of coagulative necrosis. Viable atypical cells proliferated (▲) at the interface with adjacent normal villous tissue (left side). (B) H&E staining, ×200. Atypical trophoblastic proliferation with a mixture of mononucleated cytotrophoblasts (▲) and multinucleated giant trophoblastic cells (syncytiotrophoblasts) (△). (C) Ki-67 immunostaining, ×100. A high proportion of mononuclear tumor cells showed Ki-67 positivity, indicating a high proliferative index. (D) p63 immunostaining, ×100. A subset of mononuclear tumor cells showed nuclear positivity for p63.
Figure 2. Histopathological findings of the placenta from the first pregnancy complicated by intraplacental choriocarcinoma(A) Hematoxylin and eosin (H&E) staining, ×20. The right side of the image shows a broad area of coagulative necrosis. Viable atypical cells proliferated (▲) at the interface with adjacent normal villous tissue (left side). (B) H&E staining, ×200. Atypical trophoblastic proliferation with a mixture of mononucleated cytotrophoblasts (▲) and multinucleated giant trophoblastic cells (syncytiotrophoblasts) (△). (C) Ki-67 immunostaining, ×100. A high proportion of mononuclear tumor cells showed Ki-67 positivity, indicating a high proliferative index. (D) p63 immunostaining, ×100. A subset of mononuclear tumor cells showed nuclear positivity for p63. 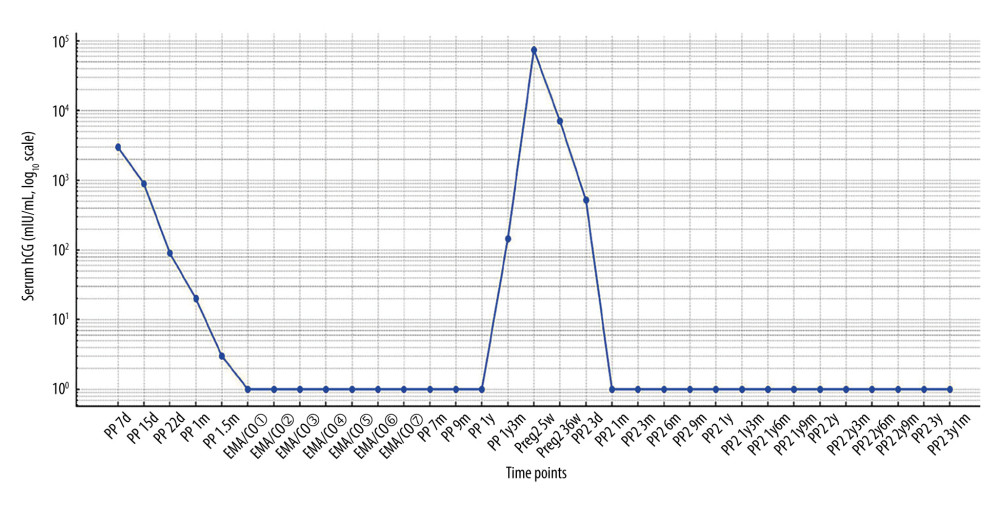 Figure 3. Temporal changes in serum human chorionic gonadotropin (hCG) levels throughout the clinical courseSerial measurements of serum hCG levels during follow-up and the subsequent pregnancy. PP – postpartum; PP2 – postpartum (second pregnancy); Preg2 – second pregnancy; d – days; w – weeks; m – months; y – years. Values plotted at 1 indicate levels below the assay detection limit (<2 mIU/mL).
Figure 3. Temporal changes in serum human chorionic gonadotropin (hCG) levels throughout the clinical courseSerial measurements of serum hCG levels during follow-up and the subsequent pregnancy. PP – postpartum; PP2 – postpartum (second pregnancy); Preg2 – second pregnancy; d – days; w – weeks; m – months; y – years. Values plotted at 1 indicate levels below the assay detection limit (<2 mIU/mL). References
1. Bruce S, Sorosky J, Gestational trophoblastic disease: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing
2. Jiao L, Ghorani E, Sebire NJ, Seckl MJ, Intraplacental choriocarcinoma: systematic review and management guidance: Gynecol Oncol, 2016; 141(3); 624-31
3. Caldas RF, Oliveira P, Rodrigues C, Intraplacental choriocarcinoma: Rare or underdiagnosed? Report of 2 cases diagnosed after an incomplete miscarriage and a preterm spontaneous vaginal delivery: Case Rep Med, 2017; 2017; 7892980
4. Sala A, Ornaghi S, Delle Marchette M, Gestational intraplacental choriocarcinoma in a term pregnancy: A case report: Cureus, 2022; 14(11); e31243
5. Seckl MJ, Sebire NJ, Berkowitz RS, Gestational trophoblastic disease: Lancet, 2010; 376(9742); 717-29
6. Dahl J, Intraplacental gestational neoplasms: A review of clinically relevant diagnostically challenging lesions: Arch Pathol Lab Med, 2024; 148(4); 398-408
7. Sebire NJ, Lindsay I, Fisher RA, Seckl MJ, Intraplacental choriocarcinoma: Experience from a tertiary referral center and relationship with infantile choriocarcinoma: Fetal Pediatr Pathol, 2005; 24(1); 21-29
8. Azizi M, Akbarzade-Jahromi M, Ghaffari P, Ramezani M, Delayed diagnosis of intraplacental choriocarcinoma in a term healthy neonate – A case report and literature review: Clin Case Rep, 2022; 10(11); e6640
9. Stabile G, Gentile RM, Carlucci S, Maternal and fetal outcomes of intraplacental choriocarcinoma complicated by fetomaternal hemorrhage: A systematic review: J Matern Fetal Neonatal Med, 2023; 36(2); 2285238
10. Soper JT, Gestational trophoblastic disease: current evaluation and management: Obstet Gynecol, 2021; 137(2); 355-70
11. Ngan HYS, Seckl MJ, Berkowitz RS, Diagnosis and management of gestational trophoblastic disease: 2021 update: Int J Gynaecol Obstet, 2021; 155(Suppl 1); 86-93
12. Bogani G, Ray-Coquard I, Mutch D, Gestational choriocarcinoma: Int J Gynecol Cancer, 2023; 33(10); 1504-14
13. Liu Y, Song X, Zhang H, Long-term outcome and fertility results of intraplacental choriocarcinoma: A retrospective study of 14 patients and literature review: Orphanet J Rare Dis, 2024; 19(1); 214
14. Sorrentino F, Silvestris T, Greco F, Massive fetomaternal hemorrhage caused by an intraplacental choriocarcinoma: Case report and review of the literature: Diagnostics (Basel), 2024; 14(21); 2454
15. Sapantzoglou I, Giourga M, Psarris A, Choriocarcinoma after term pregnancy with a subsequent successful pregnancy: A rare entity: Cureus, 2023; 15(10); e47583
16. Tranoulis A, Georgiou D, Sayasneh A, Tidy J, Gestational trophoblastic neoplasia: A meta-analysis evaluating reproductive and obstetrical outcomes after administration of chemotherapy: Int J Gynecol Cancer, 2019; 29(6); 1021-31
17. Zhu L, Song H, Yang X, Xiang Y, Pregnancy outcome of patients conceiving within one year after chemotherapy for gestational trophoblastic tumor: A clinical report of 22 cases: Chin Med J (Engl), 1998; 111(11); 1004-6
18. Aso K, Tsukimori K, Yumoto Y, Prenatal findings in a case of massive fetomaternal hemorrhage associated with intraplacental choriocarcinoma: Fetal Diagn Ther, 2009; 25(1); 158-62
19. Cioffi R, Bergamini A, Gadducci A, Reproductive outcomes after gestational trophoblastic neoplasia. A comparison between single-agent and multiagent chemotherapy: Retrospective analysis from the MITO-9 Group: Int J Gynecol Cancer, 2018; 28(2); 332-37
20. Duleba AJ, Miller D, Taylor G, Effer S, Expectant management of choriocarcinoma limited to placenta: Gynecol Oncol, 1992; 44(3); 277-80
21. Black JO, Rufforny-Doudenko I, Shehata BM, Pathologic quiz case: Third trimester placenta exhibiting infarction. Intraplacental choriocarcinoma: Arch Pathol Lab Med, 2003; 127(8); e340-42
22. Monteiro S, Burling M, Doyle H, Late diagnosis of intraplacental choriocarcinoma co-existing with fetomaternal haemorrhage causing fetal demise: A case report: Case Rep Womens Health, 2021; 31; e00341
23. She Q, Cheng Z, El-Chaar D, Intraplacental choriocarcinoma coexisting with fetomaternal hemorrhage: Case report, chemotherapy management, and literature review: Medicine (Baltimore), 2018; 97(14); e9977
24. Stafford L, McNally OM, Gibson P, Judd F, Long-term psychological morbidity, sexual functioning, and relationship outcomes in women with gestational trophoblastic disease: Int J Gynecol Cancer, 2011; 21(7); 1256-63
25. Joyce CM, Coulter J, Kenneally C, Experience of women on the Irish National Gestational Trophoblastic Disease Registry: Eur J Obstet Gynecol Reprod Biol, 2022; 272; 206-12
26. Schepisi C, Dunsmuir P, Lipsett J, Oehler MK, Intraplacental choriocarcinoma in twin pregnancy causing fetomaternal haemorrhage and single twin demise: Case report: Case Rep Oncol, 2023; 16(1); 151-56
27. Sifakis S, Koukoura O, Konstantinidou AE, Sonographic findings in severe fetomaternal transfusion: Arch Gynecol Obstet, 2010; 281(2); 241-45
28. Mari G, Deter RL, Carpenter RL, Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red-cell alloimmunization. Collaborative Group for Doppler Assessment of the Blood Velocity in Anemic Fetuses: N Engl J Med, 2000; 342(1); 9-14
29. Ghorani E, Kaur B, Fisher RA, Pembrolizumab is effective for drug-resistant gestational trophoblastic neoplasia: Lancet, 2017; 390(10110); 2343-45
30. Takano N, Takamura M, Mizuno Y, Genetic and histological analysis intraplacental choriocarcinoma: a case report: Med Mol Morphol, 2024; 57(2); 147-54
Figures
Figure 1. (A, B) Gross appearance of the placenta from the first pregnancy complicated by intraplacental choriocarcinoma. Gross examination of the placenta from the first pregnancy revealed a well-demarcated, brownish-white nodular lesion measuring 4 cm in diameter, with extensive areas of necrosis (arrows).Figure 2. Histopathological findings of the placenta from the first pregnancy complicated by intraplacental choriocarcinoma(A) Hematoxylin and eosin (H&E) staining, ×20. The right side of the image shows a broad area of coagulative necrosis. Viable atypical cells proliferated (▲) at the interface with adjacent normal villous tissue (left side). (B) H&E staining, ×200. Atypical trophoblastic proliferation with a mixture of mononucleated cytotrophoblasts (▲) and multinucleated giant trophoblastic cells (syncytiotrophoblasts) (△). (C) Ki-67 immunostaining, ×100. A high proportion of mononuclear tumor cells showed Ki-67 positivity, indicating a high proliferative index. (D) p63 immunostaining, ×100. A subset of mononuclear tumor cells showed nuclear positivity for p63.Figure 3. Temporal changes in serum human chorionic gonadotropin (hCG) levels throughout the clinical courseSerial measurements of serum hCG levels during follow-up and the subsequent pregnancy. PP – postpartum; PP2 – postpartum (second pregnancy); Preg2 – second pregnancy; d – days; w – weeks; m – months; y – years. Values plotted at 1 indicate levels below the assay detection limit (<2 mIU/mL). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133