20 December 2025: Articles 
Diagnostic Challenges of Abdominal Tumors Without Typical Imaging Features: From Misdiagnosis of Pancreatic Cystadenoma to Adrenal Pheochromocytoma and the Intraoperative Response
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents
Haoyang HuangDOI: 10.12659/AJCR.950574
Am J Case Rep 2025; 26:e950574






Abstract
BACKGROUND: Pheochromocytoma is a rare neuroendocrine tumor. Some patients are asymptomatic, and misdiagnosis is common, especially when it lacks typical imaging features. In asymptomatic patients misdiagnosed with pheochromocytoma, hemodynamic instability often occurs during surgical procedures, posing significant challenges to surgeons and anesthesiologists. This case report presents a patient who was misdiagnosed as having a pancreatic cystadenoma prior to surgery, aiming to explore the intraoperative decision-making and considerations for such cases.
CASE REPORT: A 48-year-old woman with abdominal pain was preoperatively diagnosed with pancreatic cystadenoma by imaging. Laparoscopic surgery was performed following standard procedures, including patient positioning, stomach suspension, tumor search, and tissue dissection. The surgery lasted 156 min, with minimal blood loss (50 mL). Intraoperative hemodynamic instability occurred, and the final histopathological report confirmed the tumor as a pheochromocytoma. The patient was monitored in the intensive care unit (ICU) after surgery and was discharged on the 8th postoperative day, without complications.
CONCLUSIONS: Clinicians should be aware of the limitations of imaging. When dealing with abdominal tumors lacking typical features, especially those located in the adrenal gland or para-adrenal region, a high suspicion for asymptomatic pheochromocytoma is necessary. In the event of intraoperative hemodynamic instability, a high degree of suspicion for pheochromocytoma is needed. Moreover, it is crucial to strengthen multidisciplinary collaboration and emphasize the optimization of preoperative laboratory tests and examinations to compensate for the limitations of imaging studies. Surgeons need to be prepared for unexpected findings during surgery and adjust the surgical plan according to local anatomy to improve surgical safety and success rates.
Keywords: Hemodynamic Monitoring, Laparoscopy, Pheochromocytoma, Humans, Female, Middle Aged, Adrenal Gland Neoplasms, Diagnostic Errors, Pancreatic Neoplasms, Cystadenoma, Diagnosis, Differential
Introduction
Pheochromocytoma is a rare neuroendocrine tumor, affecting approximately 19.8 per million people annually [1]. Its classic symptoms include headache, palpitation, anxiety, and diaphoresis, and it can affect people of any age, with an equal sex distribution [2]. The diagnosis of pheochromocytoma typically begins with the presence of sustained or paroxysmal hypertension [3]. However, some patients with this tumor remain asymptomatic; despite the absence of symptoms, surgery remains the first-line treatment, and their definitive diagnosis is often only confirmed postoperatively [4,5]. Asymptomatic patients often experience hypertensive crises during surgery due to preoperative misdiagnosis [6]. Thus, diagnosing and treating asymptomatic pheochromocytoma is challenging. If it lacks typical imaging features preoperatively, misdiagnosis is very likely. Video 1 presents a patient initially diagnosed with pancreatic cystadenoma by imaging before surgery. Hemodynamic disturbances occurred during the operation, and the final diagnosis turned out to be an adrenal pheochromocytoma. This article aims to highlight the diagnostic challenges and intraoperative decision-making related to asymptomatic pheochromocytomas without typical imaging features, and to discuss the surgical considerations for such cases.
Case Report
Procedure Outline
PROCEDURE OUTLINE:
On operating room entry, her vital signs were T 36.2°C, P 95 bpm, R 20 breaths/min, and BP 138/85 mmHg.
PATIENT POSITIONING AND TROCAR PLACEMENT:
For the procedure, the patient was placed in the reverse Trendelenburg position and 5 trocars were used. The chief surgeon stood on the patient’s right, the assistant on the left, and the endoscope holder stood between the patient’s legs.
SUSPENSION OF THE STOMACH AND EXPOSURE OF THE SURGICAL FIELD:
We dissected the ligaments around the stomach, and used absorbable sutures to complete the suspension of the stomach. This provided a surgical field for exposure of the pancreas and important blood vessels.
DISSECTION OF TOLDT’S SPACE AND SEARCH FOR THE TUMOR:
Approaching from below the pancreas, we dissected Toldt’s space, and located the splenic, portal, and superior mesenteric veins. We used the splenic vein as a guide to dissect the surrounding tissues toward the spleen to search for the tumor.
DISSECT THE TISSUES AROUND THE TUMOR: We dissected the tissues and blood vessels around the tumor from multiple angles. As the dissection of the tissues surrounding the tumor proceeded, it was intraoperatively identified that the tumor did not originate from the pancreas. Meanwhile, the patient had hemodynamic instability, as with a sudden blood pressure spike (Figure 2). Considering the local anatomy, we suspected it was an adrenal pheochromocytoma. The situation was then communicated to the anesthesiologist, with a simultaneous request for intraoperative consultation from the Urology Department. It was suggested that sodium nitroprusside be used to reduce blood pressure during tumor resection, and that hydrocortisone and methylprednisolone be administered concurrently with the excision of the tumor specimen. Meanwhile, norepinephrine and metaraminol were prepared to manage hypotension caused by the abrupt decrease in catecholamines following tumor resection. After that, we handled the situation in accordance with the consultation opinions, after which the tumor was progressively dissected and removed.
The surgery was successfully completed with no postoperative complications. The surgical procedure lasted 156 min, and the blood loss was extremely minimal, only 50 mL. Due to the unstable hemodynamics during the operation, she was transferred to the ICU for close monitoring and treatment after the surgery. She was discharged from the hospital 8 days after the operation. The histopathological report revealed that the mass was a pheochromocytoma. The results of immunohistochemical staining for DNA mismatch repair (MMR) proteins indicated intact mismatch repair function (pMMR), which corresponds to the microsatellite instability-low/microsatellite stable phenotype (MSI-L/MSS phenotype) (Figure 3), which indicates low genetic instability of the tumor and provides a key molecular basis for subsequent determination of the suitability of immunotherapy. One month after the surgery, the patient returned to the hospital for a follow-up CT scan, which showed good recovery. The plasma catecholamine and dihydroxyphenylglycine levels were both normal. She had no episodes of elevated blood pressure or other related conditions.
Discussion
Pheochromocytoma, a rare neuroendocrine tumor, often poses diagnostic difficulties. The classic symptoms of headache, palpitation, anxiety, and diaphoresis are not always present. In this case, the patient was asymptomatic, with no signs of hypertension-related symptoms and no history of hypertension. This lack of typical manifestations made the preoperative diagnosis based on symptoms impossible. Moreover, the initial imaging misdiagnosed the adrenal pheochromocytoma as a pancreatic cystadenoma. Pheochromocytomas typically present as relatively large tumors with regular, smooth margins, showing a round or oval mass. On contrast-enhanced scans, the lesions often exhibit marked and heterogeneous enhancement in the arterial phase, with the enhancement gradually becoming homogeneous in the portal venous phase [8–10]. However, a review of this case reveals that the central part of the lesion was cystic and non-enhancing, which is inconsistent with the conventional imaging features of pheochromocytomas, thereby leading to misdiagnosis. Cystic pheochromocytoma is a rare subtype, accounting for only 3.2% of cases [11]. Misdiagnosis of cystic tumors located in the junctional zone is not uncommon [6,8], as imaging techniques, while vital for clinical diagnosis, have limitations, especially for tumors located at organ junctions. The overlapping anatomical structures and the non-specific imaging features of pheochromocytoma can lead to such errors.
The intraoperative sudden blood pressure spike – an unexpected hemodynamic event – served as the critical clue for revising the diagnosis. Based on the tumor’s anatomical location and catecholamine-induced hemodynamic changes, pheochromocytoma was strongly suspected. Timely communication with anesthesiologists (for immediate blood pressure control via sodium nitroprusside) and emergency consultation with urologists for peri-resection medication guidance regarding hydrocortisone and prepared norepinephrine directly facilitated rapid surgical strategy adjustment [12]. This process highlights 2 core lessons: intraoperative findings inconsistent with preoperative imaging require immediate diagnostic reassessment; and multidisciplinary collaboration of the surgeon, anesthesiologist, and specialist is pivotal to managing life-threatening risks from unsuspected pheochromocytoma.
In patients with pheochromocytoma, massive catecholamine secretion can occur intraoperatively, leading to intense vascular contraction and elevated blood pressure. Preoperative administration of α-receptor blockers can dilate blood vessels, mitigate severe blood pressure fluctuations caused by massive catecholamine release, help maintain stable intraoperative blood pressure, and reduce the incidence of cardio-cerebrovascular accidents [13]. Therefore, in cases where pheochromocytoma is suspected preoperatively, we strongly recommend the use of α-receptor blockers. However, reviewing this case, none of the preoperative evidence suggested pheochromocytoma. Prophylactic use of α-receptor blockers in such scenarios can increase intraoperative bleeding and complicate anesthetic management. Thus, α-receptor blockers should not be used prophylactically when pheochromocytoma is not clearly diagnosed preoperatively.
Cystic degeneration in the central part of the tumor may have disrupted the structure of functional tumor cells, leading to a further decrease in the ability to synthesize or secrete hormones, thereby failing to induce clinical symptoms. When compared with previous cases, the hemodynamic fluctuations in our case were more significant [8]. This not only serves as an important warning signal but also is an aspect worthy of reflection. We hypothesize that in this case, the release of the cyst contents caused by intraoperative manipulation such as traction resulted in more significant hemodynamic fluctuations. Although the prognosis is somewhat unclear, the favorable outcome of our patient shows that timely, accurate diagnosis and appropriate surgical intervention are vital for the prognosis of patients with cystic pheochromocytoma.
For future clinical practice, this case has several implications. First, when dealing with abdominal tumors that lack typical imaging features, a high index of suspicion for asymptomatic pheochromocytoma should be maintained. Preoperative biochemical screening for pheochromocytoma, such as measuring urinary or plasma catecholamines and their metabolites, may be considered even in the absence of typical symptoms, especially for tumors in the adrenal or para-adrenal regions. Biochemical tests can compensate for the limitations of imaging examinations. Second, the surgical team should be well-prepared for unexpected findings during surgery. A comprehensive preoperative assessment, including a detailed review of the patient’s anatomy and a consideration of the possibility of a rare tumor, can help in formulating contingency plans. For inevitable intraoperative emergencies, multidisciplinary collaboration is very important. Close cooperation can significantly reduce the damage caused by unexpected events and ensure a safe surgery.
Conclusions
For abdominal tumors without typical imaging features, surgeons must suspect lesions in the adrenal/para-adrenal regions and incidental tumors in asymptomatic patients. Preoperatively, biochemical screening (eg, catecholamine detection) and multidisciplinary consultations should be integrated to compensate for imaging limitations. During surgery, if the tumor origin is inconsistent with preoperative findings or hemodynamic instability occurs, surgical plans should be adjusted based on anatomy and collaborative responses initiated. Postoperatively, enhanced monitoring and follow-up are essential to improve the diagnosis and safety of treatment.
Figures
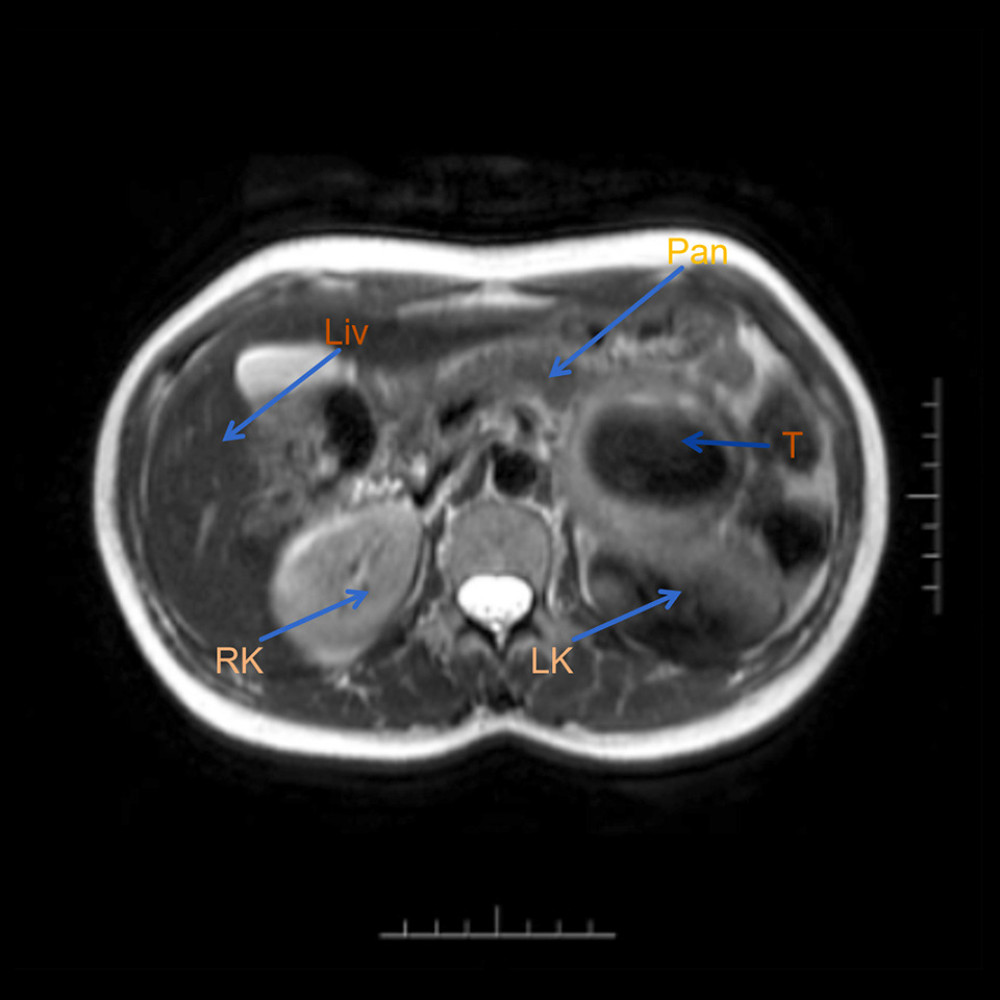 Figure 1. Preoperative MRI (RK – right kidney; LK – left kidney; T – tumor; Pan – pancreas; Liv – liver).
Figure 1. Preoperative MRI (RK – right kidney; LK – left kidney; T – tumor; Pan – pancreas; Liv – liver). 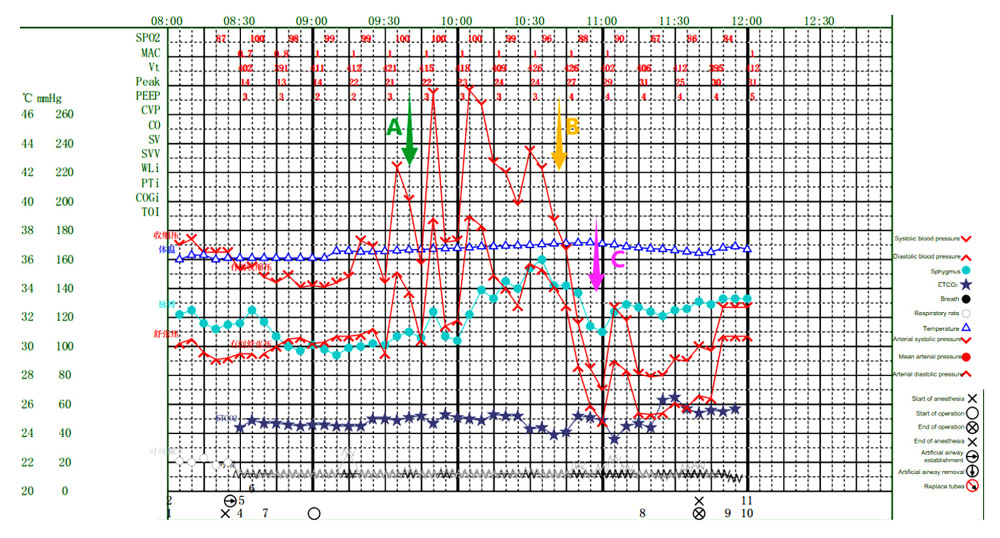 Figure 2. Intraoperative anesthesia record. A) Use sodium nitroprusside. B) Use hydrocortisone. C) Use norepinephrine and metaraminol.
Figure 2. Intraoperative anesthesia record. A) Use sodium nitroprusside. B) Use hydrocortisone. C) Use norepinephrine and metaraminol. 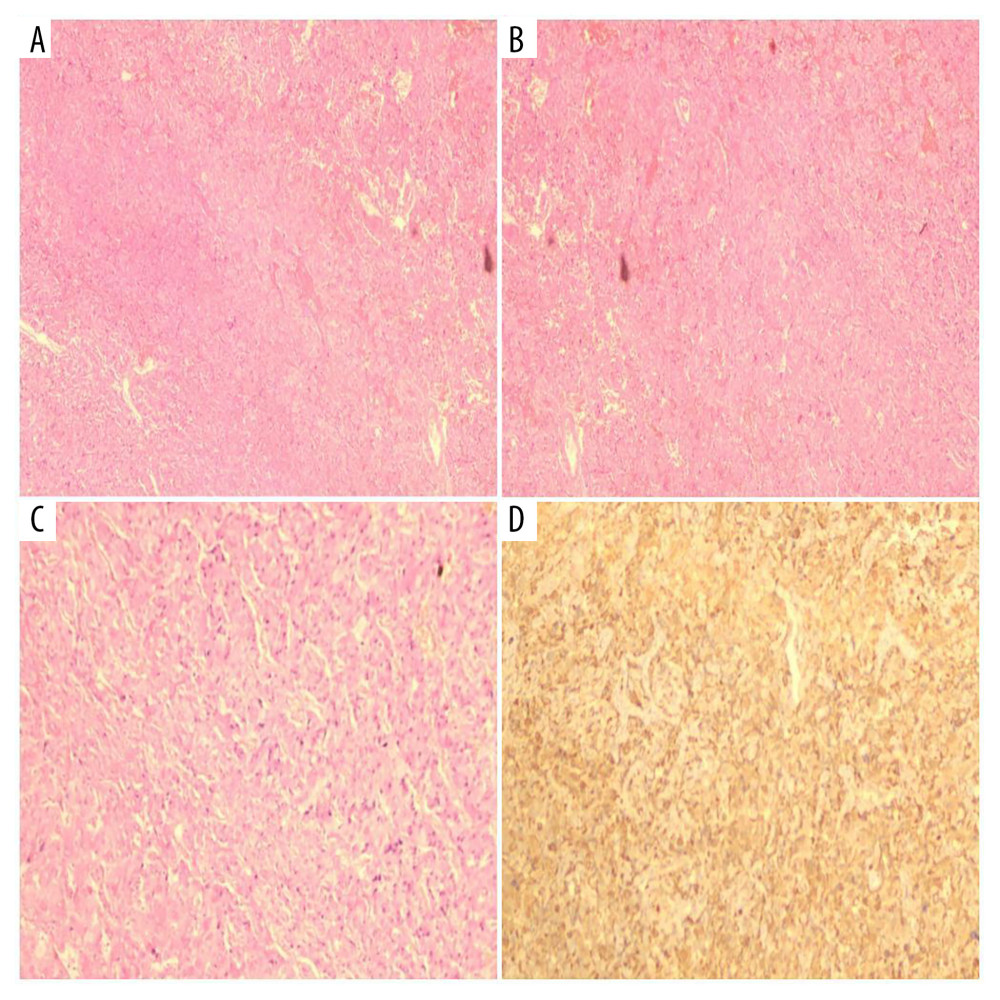 Figure 3. Pathology results showing adrenal pheochromocytoma. (A, B) Staining with hematoxylin-eosin (HE); Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=100–200 μm (low-power). (C) Staining with hematoxylin-eosin (HE); Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=25–50 μm (high-power). (D) Immunohistochemical staining; Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=25–50 μm (high-power); Immunohistochemical Results: S100(+), PMS-2 (machine-stained) (+), MLH1 (machine-stained) (focal +), MSH2 (machine-stained) (focal +), MSH6 (machine-stained) (+), β-catenin (membranous +), inhibin-α(−), Ki-67(1%), ATRX(+), SF-1 (+), P27(+), CD56(+), CgA(+), Syn(+), CKL(−), SDHB(+).
Figure 3. Pathology results showing adrenal pheochromocytoma. (A, B) Staining with hematoxylin-eosin (HE); Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=100–200 μm (low-power). (C) Staining with hematoxylin-eosin (HE); Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=25–50 μm (high-power). (D) Immunohistochemical staining; Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=25–50 μm (high-power); Immunohistochemical Results: S100(+), PMS-2 (machine-stained) (+), MLH1 (machine-stained) (focal +), MSH2 (machine-stained) (focal +), MSH6 (machine-stained) (+), β-catenin (membranous +), inhibin-α(−), Ki-67(1%), ATRX(+), SF-1 (+), P27(+), CD56(+), CgA(+), Syn(+), CKL(−), SDHB(+).  Video 1. Complete demonstration of the surgical procedure.
Video 1. Complete demonstration of the surgical procedure. References
1. Vitturi G, Crisafulli S, Alessi Y, Global epidemiology of pheochromocytoma: A systematic review and meta-analysis of observational studies: J Endocrinol Invest, 2025; 48(7); 1234-45
2. Lenders JWM, Duh QY, Eisenhofer G, Pheochromocytoma and paraganglioma: An Endocrine Society clinical practice guideline: J Clin Endocrinol Metab, 2014; 99(6); 1915-42
3. Gu YW, Poste J, Mehta K, Schwarcz M, Cardiovascular manifestations of pheochromocytoma: Cardiol Rev, 2017; 25(5); 215-22
4. Farrugia FA, Martikos G, Tzanetis P, Pheochromocytoma, diagnosis and treatment: Review of the literature: Endocr Regul, 2017; 51(3); 168-81
5. Spiro A, Usman A, Ajmal A, Asymptomatic and biochemically silent pheochromocytoma with characteristic findings on imaging: Case Rep Endocrinol, 2020; 2020; 8847261
6. Kim BC, Pak SJ, Kwon D, Silent pheochromocytoma in adrenal incidentaloma: Unveiling clinical and radiological characteristics: Ann Surg Treat Res, 2024; 106(1); 38-44
7. Li ZS, Jin ZD, Li X, Chinese diagnostic guidelines for pancreatic cystic tumors 2022: J Clin Hepatol (Chin), 2023; 39(2); 290-98
8. Zhu X, Li ZY, Guo SJ, Clinical analysis of 205 cases of adrenal pheochromocytoma/paraganglioma: J Mod Urol (Chin), 2021; 26(5); 405-9
9. Chinese Soc Endocrinol, Chinese Med Assoc, Expert consensus on the diagnosis and treatment of pheochromocytoma and paraganglioma 2020 edition: Chin J Endocrinol Metab, 2020; 36(9); 737-50
10. Leung K, Stamm M, Raja A, Low G, Pheochromocytoma: The range of appearances on ultrasound, CT, MRI, and functional imaging: Am J Roentgenol, 2013; 200(2); 370-78 [Erratum in: Am J Roentgenol. 2013;200(3):705]
11. Dogra P, Navin PJ, McKenzie TJ, Clinical, imaging and biochemical presentation of cystic pheochromocytomas: Clin Endocrinol (Oxf), 2023; 98(1); 32-40
12. Sacks GD, Shannon EM, Dawes AJ, Teamwork, communication and safety climate: A systematic review of interventions to improve surgical culture: BMJ Qual Saf, 2015; 24(7); 458-67
13. Groeben H, Nottebaum BJ, Alesina PF, Perioperative α-receptor blockade in phaeochromocytoma surgery: An observational case series: Br J Anaesth, 2017; 118(2); 182-89
Figures
Figure 1. Preoperative MRI (RK – right kidney; LK – left kidney; T – tumor; Pan – pancreas; Liv – liver).Figure 2. Intraoperative anesthesia record. A) Use sodium nitroprusside. B) Use hydrocortisone. C) Use norepinephrine and metaraminol.Figure 3. Pathology results showing adrenal pheochromocytoma. (A, B) Staining with hematoxylin-eosin (HE); Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=100–200 μm (low-power). (C) Staining with hematoxylin-eosin (HE); Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=25–50 μm (high-power). (D) Immunohistochemical staining; Observation perspective: Two-dimensional planar observation; Internal scale: 1 unit=25–50 μm (high-power); Immunohistochemical Results: S100(+), PMS-2 (machine-stained) (+), MLH1 (machine-stained) (focal +), MSH2 (machine-stained) (focal +), MSH6 (machine-stained) (+), β-catenin (membranous +), inhibin-α(−), Ki-67(1%), ATRX(+), SF-1 (+), P27(+), CD56(+), CgA(+), Syn(+), CKL(−), SDHB(+).Video 1. Complete demonstration of the surgical procedure. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133