17 December 2025: Articles 
Splenic Hamartoma Diagnosed and Treated by Laparoscopic Splenectomy Associated With a Minimal Suprapubic Approach
Challenging differential diagnosis, Unusual setting of medical care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Hikaru Ohtani BCDF 1, Tomohide Hori ABCDEF 1*, Shigeki Nakayama DF 1, Satoru Umegae DF 1, Takao Iwanaga DF 1, Ryutaro Nishikawa DF 1, Takahiro Shimoyama DF 1, Sakurako Suzuki CF 1, Shigehito Nakashima D 2, Takayuki Yamamoto ADF 1DOI: 10.12659/AJCR.950597
Am J Case Rep 2025; 26:e950597






Abstract
BACKGROUND: Splenic tumors are rare and challenging to diagnose, and laparoscopic splenectomy (LS) is useful for treatment. Splenic hamartoma is a rare benign condition that consists of disorganized normal splenic tissue, including red pulp elements, that can be asymptomatic and found incidentally.
CASE REPORT: A 42-year-old woman underwent ultrasonography, and a 70×55 mm splenic mass was detected. The tumor was composed of a solid component and a cystic lesion, and splenomegaly was observed (size: 143 mm). Contrast-enhanced computed tomography (CT) of the solid component clearly showed homogeneous and strong enhancement in the early phase. The estimated splenic volume was 650.7 mL. Magnetic resonance imaging did not indicate malignancy. A preoperative diagnosis of splenic hamartoma was made, and LS was performed. To control intraoperative bleeding and to shrink the spleen, the splenic artery was ligated first. The spleen was caught in the containment bag, and a 50 mm transverse skin incision was made cranially at the pubic bone. The stump of the splenic vein was cut within the bag, and 30 mL of blood was removed to further shrink the spleen. Next, the extremely shrunken spleen (201 g) was removed through the small abdominal incision. Histopathologically, disorganized normal splenic tissue, including red pulp elements, were observed. The patient was discharged on postoperative day 4, and rehabilitation was accomplished by postoperative day 7. No postoperative complications were observed.
CONCLUSIONS: This report highlights the rare condition of splenic hamartoma, and described the key techniques for advantageous LS.
Keywords: Diagnosis, general surgery, Laparoscopy, Splenectomy, Splenic Artery, Humans, Female, Hamartoma, adult, Splenic Diseases, Tomography, X-Ray Computed
Introduction
Splenic hamartoma is a rare benign condition that consists of disorganized normal splenic tissue, including red pulp elements, that can be asymptomatic and found incidentally. Cystic spaces can be present, and hemorrhage can occur spontaneously or due to trauma [1–3]. Splenic solid tumors are rare [1] and pose a differential diagnostic challenge, especially as an incidental imaging finding. Generally, these rare tumors can be challenging to diagnose and differentiate [2,3].
The laparoscopic splenectomy (LS) was first performed in 1991 [4] and became widespread in the 1990s [5]. The feasibility and safety of this procedure have been verified; therefore, LS is a powerful tool for the treatment of splenic diseases, including hematological disorders and splenic solid tumors [1].
From the viewpoint of incidence, presentation, diagnosis, clinical course, and management of splenic hamartoma, splenic hamartoma is rare benign tumor that presents a diagnostic challenge and is usually an asymptomatic incidental finding [1–3]. This slow-growing tumor is commonly treated by surgery [1–4]. Similar cases had been previously reported [6,7].
This report describes the case of a 42-year-old woman with a solitary splenic hamartoma managed with LS using anticipatory inflow cutoff, in-bag blood removal, and a minimal suprapubic approach. The imaging findings of the splenic hamartoma and our techniques in LS are provided in detail. Additionally, we discuss the key advantages of our surgical approach and provide a review of relevant literature.
Case Report
A 42-year-old woman with Graves disease developed left-sided back pain and epigastric discomfort and was referred to our hospital. Conventional blood examination showed no abnormal findings. Free triiodothyronine, free thyroxine, and thyroid-stimulating hormone concentrations were within the respective normal ranges. Plain ultrasonography (US) was performed as a routine survey, and a hypoechoic mass measuring 70×55 mm in size was detected in the spleen (Figure 1). This regularly shaped mass consisted of both solid and cystic components. The solid component showed hypervascularity with Doppler US (Figure 1E, 1F), and splenomegaly was observed, at 143×65 mm. The patient had a history of acute bronchitis 6 years earlier and underwent thoracic plain computed tomography (CT) at another hospital, which retrospectively revealed a small (13 mm) splenic mass (Figure 2).
Plain CT at our hospital revealed that the solid component appeared as a low-density mass, similar to the findings 6 years earlier. Dynamic contrast-enhanced CT clearly showed homogeneous and strong enhancement in the early phase, with strong and prolonged enhancement in later phases (Figure 3). An accessory spleen was not observed, and collateral vessels were visible around the splenic hilum. Three-dimensional images were also obtained (Figure 4A, 4B), and the estimated splenic volume was 650.7 mL, with CT volumetry.
T2-weighted magnetic resonance imaging (MRI) showed that the solid component and cystic lesion both showed relatively high intensity (Figures 4C and 5A, 5B). Neither the opposed-phase- (Figure 5C, 5D) nor the in-phase (Figure 5E, 5F) gradient-echo sequence T1-weighted images could detect the solid component. T2-weighted and high-b-value diffusion-weighted imaging (range: 0–800 s/mm2) revealed no positive enhancement in the solid component (Figure 6A–6D), and this component had no signal suppression in the apparent diffusion coefficient map (Figure 6E, 6F).
A preoperative diagnosis of splenic hamartoma was made, although hemangioma was another possible diagnosis. Laparoscopic surgery was performed, and the port placement and skin incision are shown in Figure 7A. An incision was created in the umbilicus for the camera port, and 3 working ports were placed. Intraoperatively, a large tumor was observed in the spleen. The splenic artery and splenic vein were respectively identified using intraoperative US and then dissected and skeletonized distally (Figure 7B, 7C). To control intraoperative bleeding from the spleen and to shrink the spleen for subsequent removal through the abdominal wall, the splenic artery was ligated using a clip and then cut using laparoscopic coagulation shears (Figure 7D, 7E). Next, the splenic vein was ligated and cut. Finally, the spleen was mobilized from the retroabdominal space by cutting the connective tissue (Figure 7F) and caught in the containment bag (Figure 8A). A transverse skin incision measuring 50 mm in length was made cranially at the pubic bone (Figure 7A). The mouth of the containment bag was introduced extraperitoneally through the suprapubic incision in the abdominal wall, and the bag was subsequently opened. The stump of the splenic vein was cut within the bag, and blood in the resected spleen was removed to further shrink the spleen. A total of 30 mL of blood was removed (Figure 8B). Next, the extremely shrunken spleen (maximum original size: 143 mm) was removed through the abdominal incision. The weight of the resected specimen was 201 g, although the estimated splenic volume was 650.7 mL (approximately, 651 g). An intraperitoneal drain was placed at the left subphrenic space through the port incision (Figure 8C). The operative time was 106 min, and intraoperative blood loss was 30 mL.
Macroscopically, the splenic tumor consisted of a solid component and a cystic lesion, as indicated in the preoperative imaging findings (Figure 9A, 9B). The solid component was soft on palpation. Splenic hamartoma is a rare benign condition of the spleen that consists of disorganized normal splenic tissue, including red pulp elements in sinuses and cords, without any white pulp component. The definitive diagnosis of splenic hamartoma was made histopathologically (Figure 9C, 9D).
The patient was discharged on postoperative day 4, and rehabilitation was accomplished by postoperative day 7. Postoperatively, the maximum platelet count was 39×104/μL, and the patient received a pneumococcal vaccination (Prevenar; Pfizer Inc, NY, NY, USA). No hemorrhage, thrombosis, or infections were observed, postoperatively, and the patient was in good health 1 year after laparoscopic surgery.
Discussion
In this article, we showed image findings of our patient in detail, and demonstrated our technical approach to improve the advantages of LS, though case reports always have the limitation of study.
Solitary splenic masses are rare, and most are eventually diagnosed as malignant tumors, including non-Hodgkin lymphoma. The most common benign lesion is inflammatory pseudotumor [1]. In our case, homogeneous strong enhancement of the solid component in the early phase of dynamic contrast-enhanced CT was observed, and MRI findings did not suggest malignancy. Thus, we made a preoperative diagnosis of splenic hamartoma. Regarding the therapeutic strategy, in similar cases, the presence of an accessory spleen should be carefully checked during imaging before LS [8,9].
Although adequate therapeutic strategy of splenic hamartoma should be made based on definitive diagnosis, establishing such a diagnosis for this rare splenic tumor can be challenging for physicians in gastroenterology and general surgery [1–3]. LS is considered an adequate treatment for splenic hamartoma and a strong tool for making definitive diagnosis based on histopathological assessment [1,5].
Splenectomy was first performed for therapeutic purposes by Wells in 1887 [10], and thereafter, this surgery became the criterion standard treatment in elective cases and for suitable patients [1,4]. Since Delaitre and Maignien first introduced LS in 1991 [4], this surgery has become widespread [5]. Laparoscopic surgery has many benefits specific to this approach, with several advantages over open surgery, including shorter hospital stay, lower infection rates, reduced postoperative pain, and earlier rehabilitation [11–13]. Even though LS appears to be well established [1], key points remain to increase the advantages of LS.
In this article, we demonstrated our technical approach to improve the advantages of LS. First, to control intraoperative bleeding from the spleen and to shrink the spleen for subsequent removal through the abdominal wall, the splenic artery was ligated first, while preserving splenic drainage (ie, the splenic vein and collateral vessels) (Figure 7D, 7E). This approach of anticipatory inflow cutoff (ie, an “splenic artery first” approach) drastically shrunk the spleen. Next, blood within the spleen in the containment bag was intentionally removed via the opened stump of the splenic vein. This manipulation (ie, in-bag blood removal) further shrunk the spleen before transabdominal removal of the resected specimen (Figure 8B). Therefore, anticipatory inflow cutoff and in-bag blood removal dramatically shrunk the spleen intraoperatively, from the estimated volume of 650.7 mL (approximately 651 g) to an actual weight of 201 g. Finally, a small transverse skin incision measuring 50 mm was made cranially at the pubic bone (Figures 7A and 8C). In our case, the small transabdominal incision was sufficient for removal of the extremely shrunken spleen, which had a maximum preoperative dimension of 143 mm. Compared with a large incision, a small suprapubic incision for transabdominal removal of the resected specimen is advantageous because it leads to a shorter hospital stay, less postoperative pain, and earlier rehabilitation [11]. In fact, our patient was discharged from the hospital on postoperative day 4 and returned to work on postoperative day 7. Moreover, a small suprapubic incision has cosmetic advantages because the eventual scar is fully hidden by clothing.
The spleen is an important organ and plays a vital role in both the hematologic and immune systems [4]. The spleen is the largest secondary lymphoid organ and plays an active role in homeostasis, blood filtration, and hematopoiesis. Platelet counts often increase after splenectomy [14,15], and thrombocytosis and thrombopenia can cause severe complications, such as infarction and hemorrhage [15,16]. Although the platelet count after LS in our case remained within the reference range, thrombocytosis and thrombopenia should be evaluated after LS.
The spleen is also crucial for proper immune system function and plays an active role in cellular and humoral immunity [4]. Overwhelming postoperative infections after splenectomy can progress quickly from a mild flulike illness to fulminant sepsis [17]. The need to preserve as much of the spleen as possible has been documented [18,19]; however, laparoscopic partial/subtotal splenectomy requires technically advanced surgical skills [18]. The large tumor in our case occupied the splenic parenchyma; therefore, we did not choose partial, or subtotal, splenectomy, which is associated with a wide transection surface and high bleeding risk.
Splenic solid tumors are rare, and the imaging findings in our case are described in detail in this report. LS is a valuable technique for both treating splenic tumors and making a definitive diagnosis, and we present useful technical aspects to enhance the advantages of LS. We anticipate that this case report will be informative for clinicians in the field of gastrointestinal and hepatobiliary pancreatic surgery.
Conclusions
This report highlights the rare condition of splenic hamartoma and describes key techniques that enhance the effectiveness of LS.
Figures
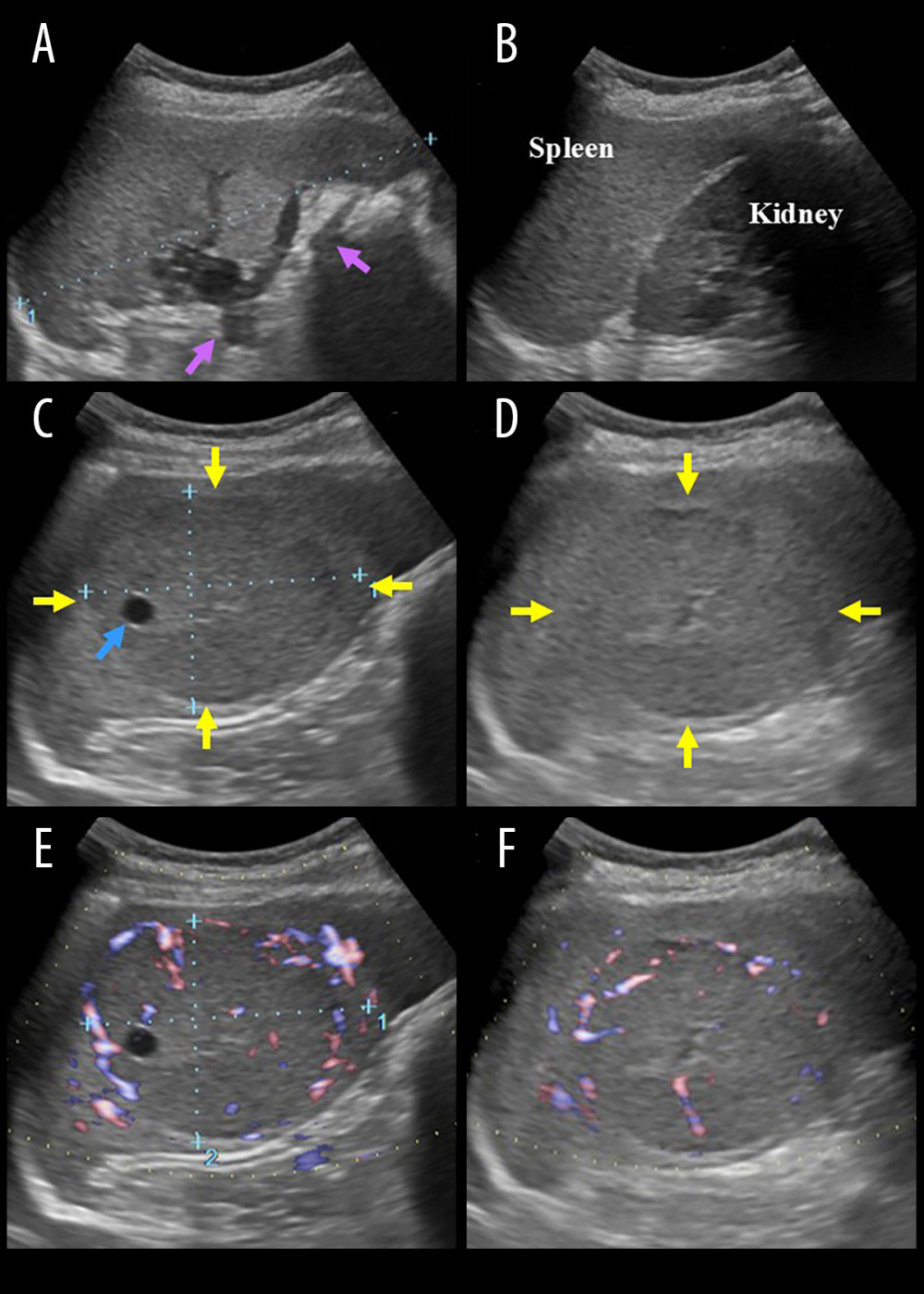 Figure 1. Ultrasonography findingsCollateral vessels were seen (A, purple arrows), and splenomegaly (143×65 mm) was observed (B). A hypoechoic splenic mass measuring 70×55 mm was detected incidentally (C, D, yellow arrows). This regularly shaped lesion involved a cystic component (C, blue arrow). The solid component showed hypervascularity with Doppler ultrasonography (E, F).
Figure 1. Ultrasonography findingsCollateral vessels were seen (A, purple arrows), and splenomegaly (143×65 mm) was observed (B). A hypoechoic splenic mass measuring 70×55 mm was detected incidentally (C, D, yellow arrows). This regularly shaped lesion involved a cystic component (C, blue arrow). The solid component showed hypervascularity with Doppler ultrasonography (E, F). 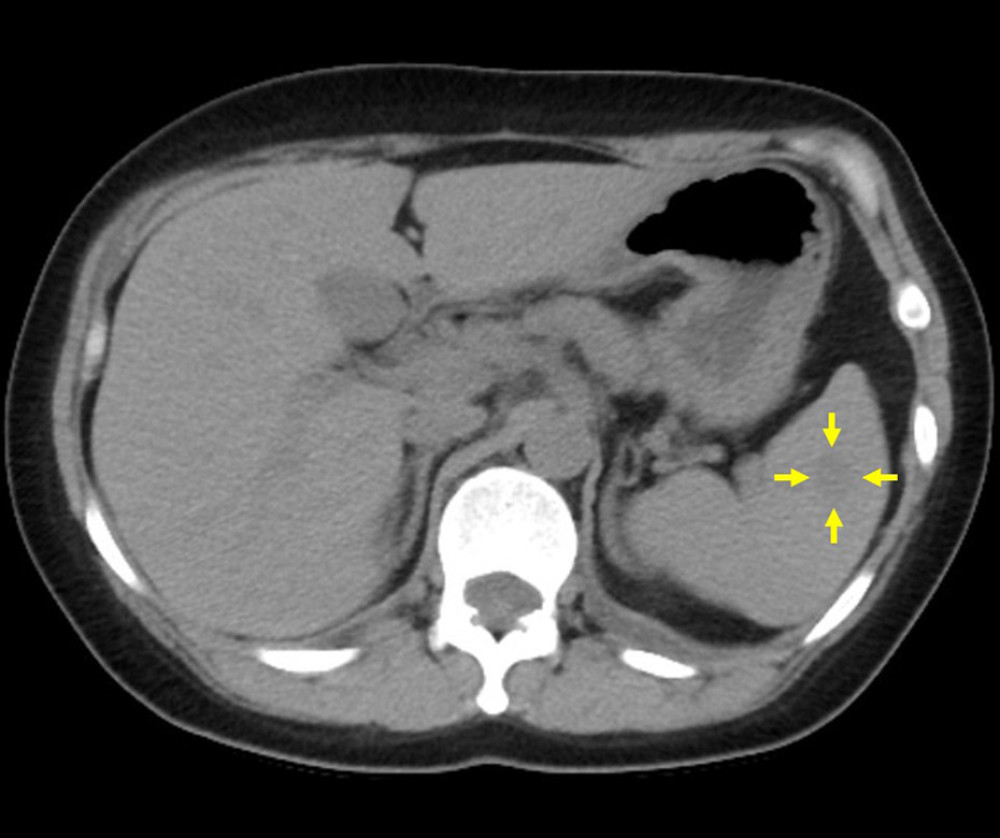 Figure 2. Tumor size during imaging performed 6 years prior to presentation at our hospitalThe splenic mass measured 13 mm 6 years prior to presentation at our hospital (yellow arrows). The blue arrow indicates the cystic lesion.
Figure 2. Tumor size during imaging performed 6 years prior to presentation at our hospitalThe splenic mass measured 13 mm 6 years prior to presentation at our hospital (yellow arrows). The blue arrow indicates the cystic lesion. 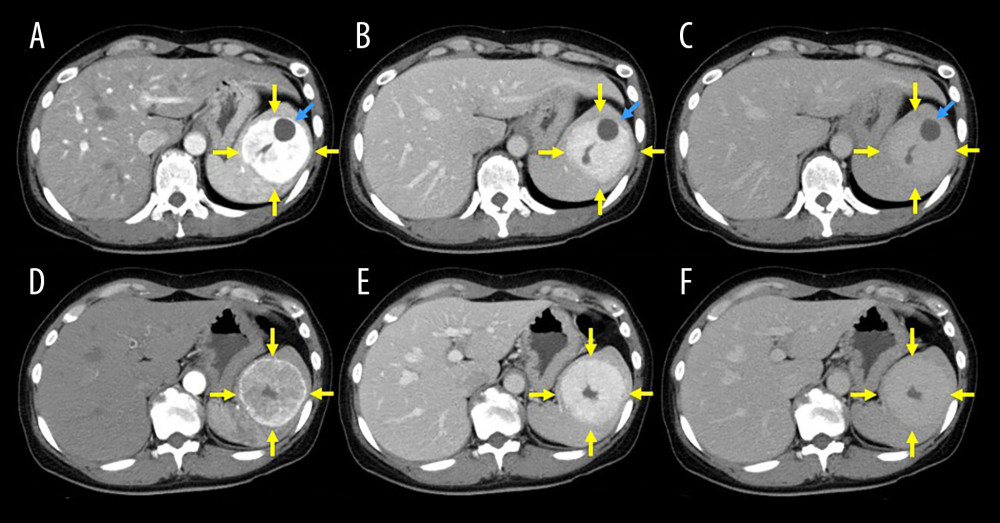 Figure 3. Contrast-enhanced computed tomography findingsThe splenic tumor consisted of a solid component (yellow arrows) and a cystic lesion (blue arrows). Imaging clearly shows homogeneous and strong enhancement in the early phase (A, B, D, E), with prolonged strong enhancement in later phases (C, F).
Figure 3. Contrast-enhanced computed tomography findingsThe splenic tumor consisted of a solid component (yellow arrows) and a cystic lesion (blue arrows). Imaging clearly shows homogeneous and strong enhancement in the early phase (A, B, D, E), with prolonged strong enhancement in later phases (C, F). 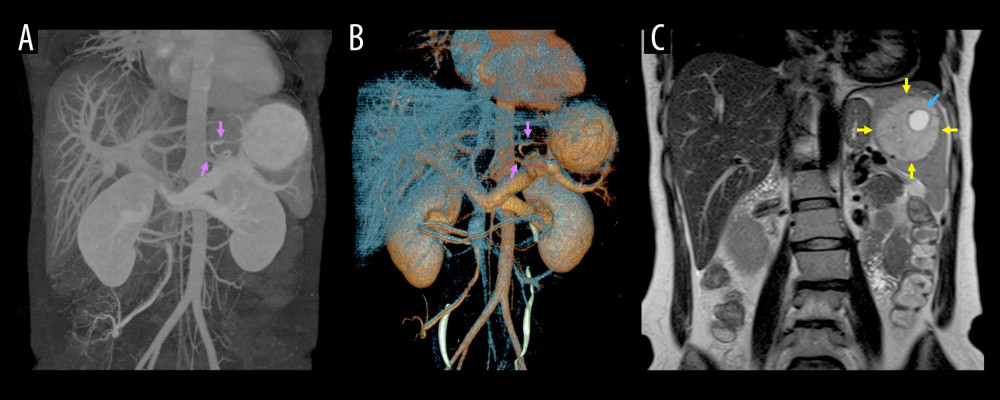 Figure 4. Three-dimensional magnetic resonance imaging findingsThe estimated splenic volume was 650.7 mL with computed tomography volumetry. Collateral vessels are visible around the splenic hilum (A, B, purple arrows). In T2-weighted imaging, the solid component (yellow arrows) and cystic lesion (blue arrow) both show relatively high intensity (C).
Figure 4. Three-dimensional magnetic resonance imaging findingsThe estimated splenic volume was 650.7 mL with computed tomography volumetry. Collateral vessels are visible around the splenic hilum (A, B, purple arrows). In T2-weighted imaging, the solid component (yellow arrows) and cystic lesion (blue arrow) both show relatively high intensity (C). 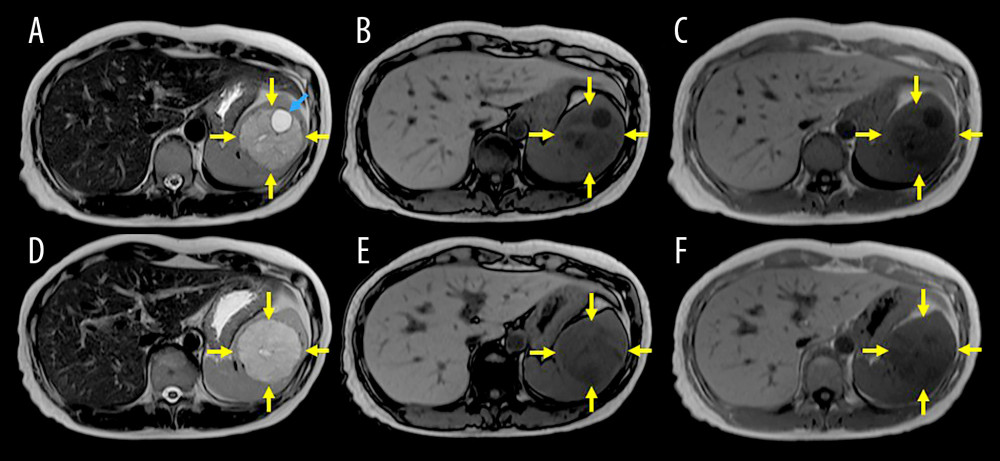 Figure 5. Magnetic resonance imaging findingsIn T2-weighted imaging, the solid component (yellow arrows) and cystic lesion (blue arrow) both show relatively high intensity (A, B). In T1-weighted imaging gradient-echo sequences, neither the opposed-phase (C, D) nor the in-phase (E, F) show the solid component.
Figure 5. Magnetic resonance imaging findingsIn T2-weighted imaging, the solid component (yellow arrows) and cystic lesion (blue arrow) both show relatively high intensity (A, B). In T1-weighted imaging gradient-echo sequences, neither the opposed-phase (C, D) nor the in-phase (E, F) show the solid component. 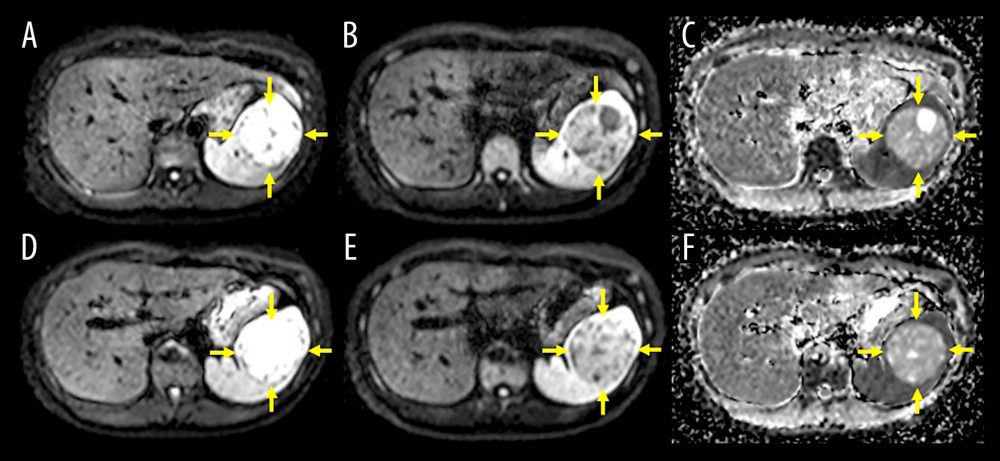 Figure 6. T2-weighted and high b-factor diffusion-weighted magnetic resonance imaging findingsImages (b-values 0–800 s/mm2) demonstrate no positive enhancement in the solid component of the lesion (A–D, yellow arrows).The solid component also shows no signal suppression in the apparent diffusion coefficient map (E, F, yellow arrows).
Figure 6. T2-weighted and high b-factor diffusion-weighted magnetic resonance imaging findingsImages (b-values 0–800 s/mm2) demonstrate no positive enhancement in the solid component of the lesion (A–D, yellow arrows).The solid component also shows no signal suppression in the apparent diffusion coefficient map (E, F, yellow arrows). 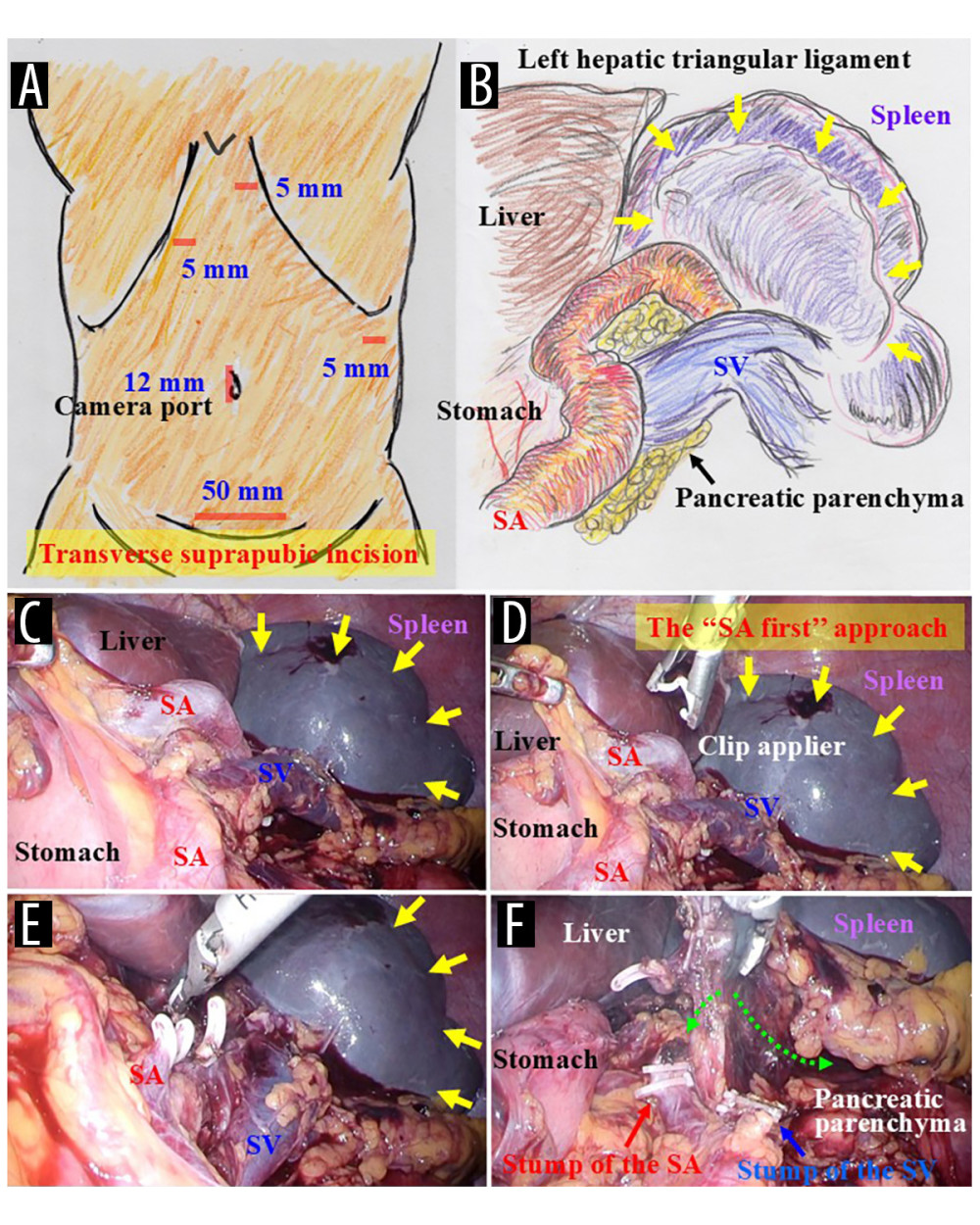 Figure 7. Initial surgical proceduresAn incision was created in the umbilicus for the camera port, and 3 working ports were placed (A). A large splenic tumor is visible intraoperatively (B–E, yellow arrows). The splenic artery (SA) and splenic vein (SV) were both skeletonized distally (B, C). To control intraoperative bleeding from the spleen and to shrink the spleen for subsequent removal through the abdominal wall, the SA was ligated before the SV (D, E). The spleen was mobilized from the retroabdominal space by cutting the connective tissue (F, green dotted arrows).
Figure 7. Initial surgical proceduresAn incision was created in the umbilicus for the camera port, and 3 working ports were placed (A). A large splenic tumor is visible intraoperatively (B–E, yellow arrows). The splenic artery (SA) and splenic vein (SV) were both skeletonized distally (B, C). To control intraoperative bleeding from the spleen and to shrink the spleen for subsequent removal through the abdominal wall, the SA was ligated before the SV (D, E). The spleen was mobilized from the retroabdominal space by cutting the connective tissue (F, green dotted arrows). 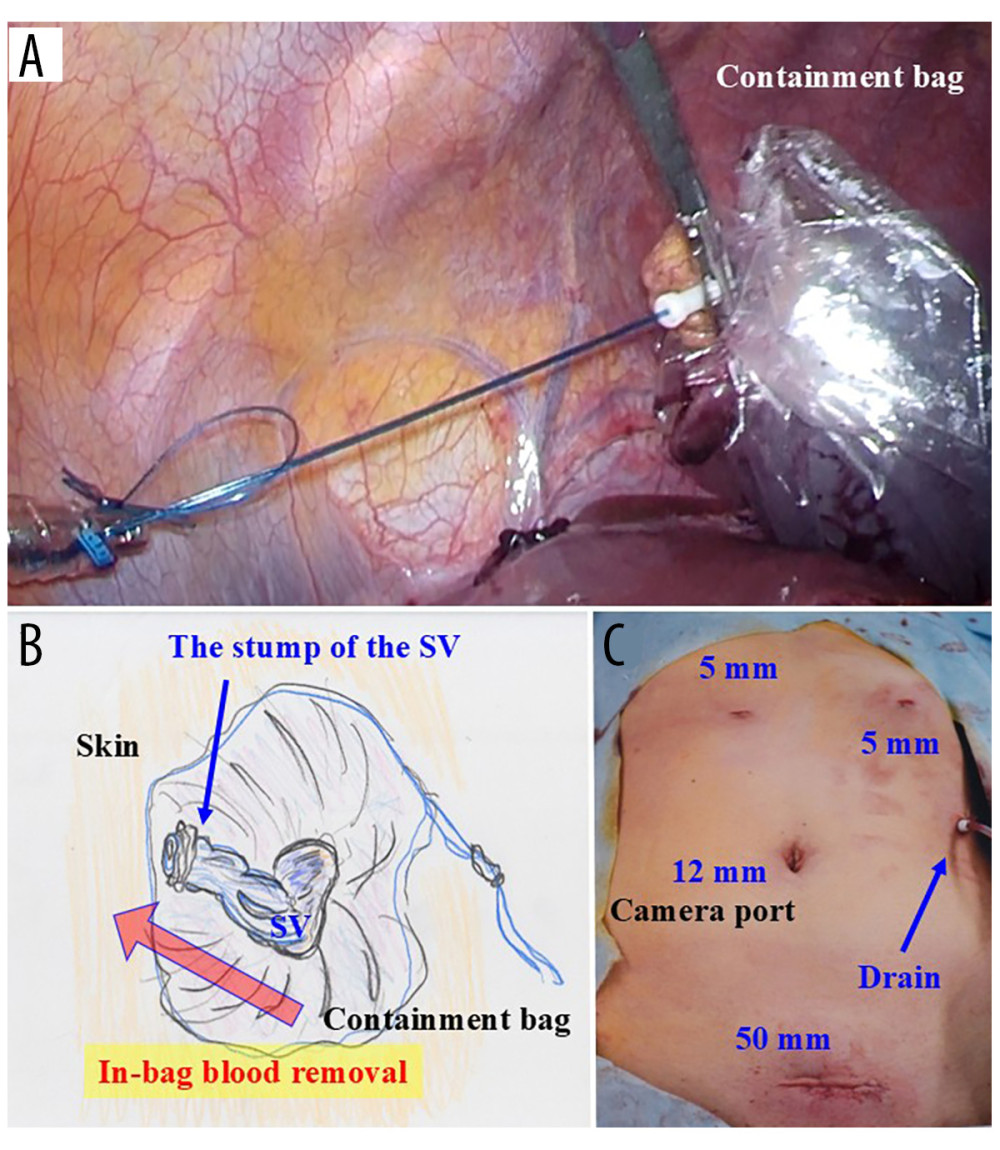 Figure 8. Additional surgical proceduresThe spleen was caught in the containment bag (A). A transverse skin incision was made cranially at the pubic bone, and the mouth of the containment bag was introduced extraperitoneally through the abdominal wall. The containment bag was opened, and the stump of the splenic vein (SV) was cut within the bag (B). Blood in the resected spleen was then removed to further shrink the spleen, and an intraperitoneal drain was placed through the port incision (C).
Figure 8. Additional surgical proceduresThe spleen was caught in the containment bag (A). A transverse skin incision was made cranially at the pubic bone, and the mouth of the containment bag was introduced extraperitoneally through the abdominal wall. The containment bag was opened, and the stump of the splenic vein (SV) was cut within the bag (B). Blood in the resected spleen was then removed to further shrink the spleen, and an intraperitoneal drain was placed through the port incision (C). 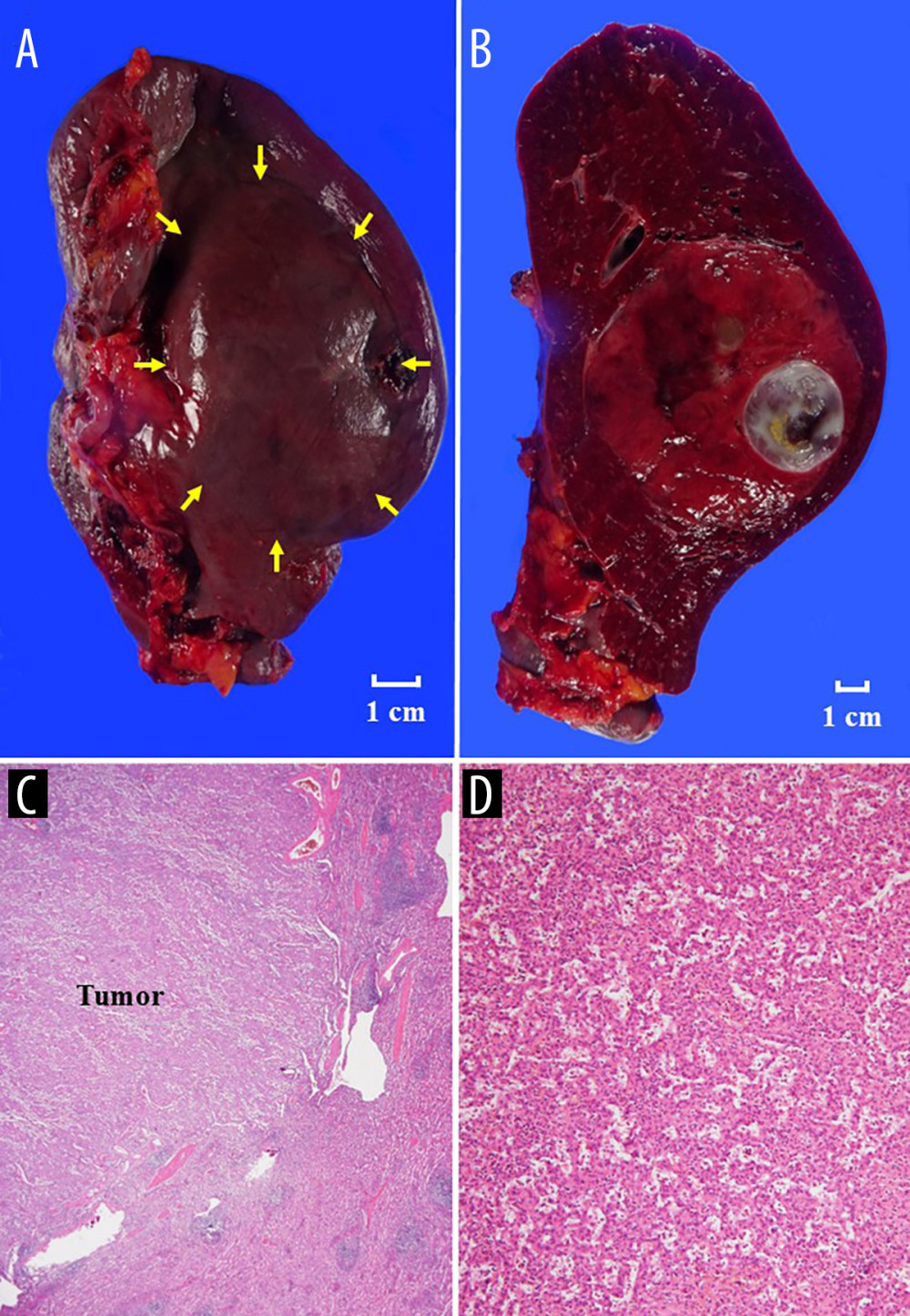 Figure 9. Histopathological findingsThe splenic tumor (yellow arrows) consisted of a solid component and a cystic lesion (A, B). Histopathological findings are shown with hematoxylin and eosin staining at ×40 (C) and ×200 (D) magnification. A mixture of unorganized vascular channels and fibrotic cords of splenic red pulp-like area were clearly observed in hematoxylin and eosin stain (D).
Figure 9. Histopathological findingsThe splenic tumor (yellow arrows) consisted of a solid component and a cystic lesion (A, B). Histopathological findings are shown with hematoxylin and eosin staining at ×40 (C) and ×200 (D) magnification. A mixture of unorganized vascular channels and fibrotic cords of splenic red pulp-like area were clearly observed in hematoxylin and eosin stain (D). References
1. Makrin V, Avital S, White I, Laparoscopic splenectomy for solitary splenic tumors: Surg Endosc, 2008; 22(9); 2009-12
2. Riller Q, Cohen-Aubart F, Roos-Weil DSplenic lymphoma, diagnosis and treatment: Rev Med Interne, 2022; 43(10); 608-16 [in French]
3. Carboni F, Federici O, Covello R, Solid tumor of the spleen: A challenging diagnosis: Surgery, 2022; 171(6); e25-e26
4. Erten E, Ucaner B, Cimen S, Retrospective investigation of patients undergoing splenectomy: Our 8-year clinical experience in a single center: North Clin Istanb, 2025; 12(2); 231-38
5. Demeure MJ, Frantzides CT, Early experience with laparoscopic splenectomy: WMJ, 1998; 97(10); 33-34
6. Sim J, Ahn HI, Han H, Splenic hamartoma: A case report and review of the literature: World J Clin Cases, 2013; 1(7); 217-19
7. Obeidat KA, Afaneh MW, Al-Domaidat HM, Splenic hamartoma: A case report and literature review: Am J Case Rep, 2022; 23; e937195
8. Meng M, Choi PJK, Pydi R, Farkas DT, Evaluating the effectiveness of laparoscopic removal of an accessory spleen after a failed splenectomy for immune thrombocytopenia: Cureus, 2024; 16(7); e65876
9. He YF, Qi SQ, Bian J, Post-splenectomy accessory spleen hyperfunction in children with hereditary spherocytosis: A rare case report and literature review: Front Pediatr, 2025; 13; 1572397
10. Silecchia G, Boru CE, Fantini A, Laparoscopic splenectomy in the management of benign and malignant hematologic diseases: JSLS, 2006; 10(2); 199-205
11. Samstein B, Griesemer A, Cherqui D, Fully laparoscopic left-sided donor hepatectomy is safe and associated with shorter hospital stay and earlier return to work: A comparative study: Liver Transpl, 2015; 21(6); 768-73
12. Rescorla FJ, Laparoscopic splenectomy: Semin Pediatr Surg, 1998; 7(4); 207-12
13. Feldman LS, Laparoscopic splenectomy: standardized approach: World J Surg, 2011; 35(7); 1487-95
14. Jeon C, Sung K, Cho J, A case report of postsplenectomy reactive thrombocytosis leading to an acute myocardial infarction in a previously healthy adult without hematologic comorbidities: Medicine (Baltimore), 2025; 104(19); e42459
15. Maehira H, Tani M, Mori H, Long-term outcomes after spleen-preserving distal pancreatectomy with splenic vessels preservation or resection: A nationwide survey of the Japanese Society of Pancreatic Surgery: Surgery, 2024; 175; 1570-79
16. Hosoda K, Shimizu A, Kubota K, A focal extramedullary hematopoiesis of the spleen in a patient with essential thrombocythemia presenting with a complicated postoperative course: A case report: Surg Case Rep, 2021; 7(1); 33
17. Sinwar PD, Overwhelming post splenectomy infection syndrome – review study: Int J Surg, 2014; 12(12); 1314-16
18. Izquierdo C, García-Picazo A, Rodríguez JP, Laparoscopic subtotal splenectomy: A feasible option in the treatment of splenic metastasis: Ann Surg Oncol, 2025; 32(2); 1232-35
19. O’Sullivan JL, Walker P, Navadgi S, Laparoscopic upper pole partial splenectomy for a complex splenic cyst with selective clamping of the magistral blood supply-A case report: J Surg Case Rep, 2025; 2025(3); rjaf183
Figures
Figure 1. Ultrasonography findingsCollateral vessels were seen (A, purple arrows), and splenomegaly (143×65 mm) was observed (B). A hypoechoic splenic mass measuring 70×55 mm was detected incidentally (C, D, yellow arrows). This regularly shaped lesion involved a cystic component (C, blue arrow). The solid component showed hypervascularity with Doppler ultrasonography (E, F).Figure 2. Tumor size during imaging performed 6 years prior to presentation at our hospitalThe splenic mass measured 13 mm 6 years prior to presentation at our hospital (yellow arrows). The blue arrow indicates the cystic lesion.Figure 3. Contrast-enhanced computed tomography findingsThe splenic tumor consisted of a solid component (yellow arrows) and a cystic lesion (blue arrows). Imaging clearly shows homogeneous and strong enhancement in the early phase (A, B, D, E), with prolonged strong enhancement in later phases (C, F).Figure 4. Three-dimensional magnetic resonance imaging findingsThe estimated splenic volume was 650.7 mL with computed tomography volumetry. Collateral vessels are visible around the splenic hilum (A, B, purple arrows). In T2-weighted imaging, the solid component (yellow arrows) and cystic lesion (blue arrow) both show relatively high intensity (C).Figure 5. Magnetic resonance imaging findingsIn T2-weighted imaging, the solid component (yellow arrows) and cystic lesion (blue arrow) both show relatively high intensity (A, B). In T1-weighted imaging gradient-echo sequences, neither the opposed-phase (C, D) nor the in-phase (E, F) show the solid component.Figure 6. T2-weighted and high b-factor diffusion-weighted magnetic resonance imaging findingsImages (b-values 0–800 s/mm2) demonstrate no positive enhancement in the solid component of the lesion (A–D, yellow arrows).The solid component also shows no signal suppression in the apparent diffusion coefficient map (E, F, yellow arrows).Figure 7. Initial surgical proceduresAn incision was created in the umbilicus for the camera port, and 3 working ports were placed (A). A large splenic tumor is visible intraoperatively (B–E, yellow arrows). The splenic artery (SA) and splenic vein (SV) were both skeletonized distally (B, C). To control intraoperative bleeding from the spleen and to shrink the spleen for subsequent removal through the abdominal wall, the SA was ligated before the SV (D, E). The spleen was mobilized from the retroabdominal space by cutting the connective tissue (F, green dotted arrows).Figure 8. Additional surgical proceduresThe spleen was caught in the containment bag (A). A transverse skin incision was made cranially at the pubic bone, and the mouth of the containment bag was introduced extraperitoneally through the abdominal wall. The containment bag was opened, and the stump of the splenic vein (SV) was cut within the bag (B). Blood in the resected spleen was then removed to further shrink the spleen, and an intraperitoneal drain was placed through the port incision (C).Figure 9. Histopathological findingsThe splenic tumor (yellow arrows) consisted of a solid component and a cystic lesion (A, B). Histopathological findings are shown with hematoxylin and eosin staining at ×40 (C) and ×200 (D) magnification. A mixture of unorganized vascular channels and fibrotic cords of splenic red pulp-like area were clearly observed in hematoxylin and eosin stain (D). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133