18 December 2025: Articles 
Plastic Corneal Foreign Body Removal From a 2-Month-Old Infant: A Case Report
Unusual clinical course, Mistake in diagnosis, Management of emergency care
Shichun Chen ABE 1, Ning Zhang BCDE 1, Huangpei Xu ABD 1, Zhichao Cai BC 1, Liangwen Li ADEF 1, Suqian Wu ABCDEF 1,2*DOI: 10.12659/AJCR.950663
Am J Case Rep 2025; 26:e950663






Abstract
BACKGROUND: Infantile corneal foreign bodies (CFBs) are rare and frequently result in delayed diagnoses and treatment challenges. This report describes a case of a very young infant with a small plastic CFB that was successfully removed.
CASE REPORT: A 2-month-old boy was observed to have a “small dot” foreign body on his left cornea by his parents. No crying response to the CFB or other symptoms had ever been identified. Slit lamp examination revealed the presence of a small, oval, plastic foreign body in the corneal epithelial layer. This CFB was determined to be an ornament affixed to the dress that the babysitter was wearing at the time. For CFB removal, medical sedation was rejected by the infant’s guardian. The initial attempt to flush the CFB out with saline or extract the CFB using a cotton-tipped applicator alone proved unsuccessful. Subsequent release of the CFB from the cornea was facilitated by the addition of proparacaine hydrochloride drops to the conjunctival sac and the use of a 1-mL needle, which was then adhered to the cotton-tipped applicator, thereby enabling its removal.
CONCLUSIONS: CFBs in young infants may not manifest any symptoms and thus can be easily ignored. The removal of plastic CFBs in those young infants who exhibit limited communication and cooperation abilities remains a challenging procedure. This report proposes a viable and low-risk, office-based approach to address the issue of CFB removal in infants.
Keywords: Emergency Medicine, Ophthalmology, Pediatrics, Traumatology, Humans, Male, Infant, Eye Foreign Bodies, Corneal Injuries, Plastics
Introduction
Corneal foreign bodies (CFBs) are a prevalent cause of ocular trauma, often regarded as an occupational hazard [1]. Approximately 8% of emergency department visits are due to eye trauma, with 31% of these cases involving CFBs [2]. Symptoms of a CFB often include pain, foreign body sensation, tearing, and/or bulbar redness [3]. CFBs can result from environmental exposure or accidental trauma, with dust, metal shavings, and organic matter being common sources, and the incidence of plastic orbital foreign body has recently increased [4]. Moreover, CFBs in young children are increasingly concerning due to the vulnerability of their developing ocular structures and the challenges in communicating symptoms [5–7].
Despite the abundance of literature on this subject and its relatively straightforward diagnosis [8–10], CFBs can be initially overlooked, particularly in young infants. In addition, treating CFBs in infants frequently poses challenging. This report describes the case of a 2-month-old boy with a small plastic CFB successfully removed by needle extraction.
Case Report
A 2-month-old boy was admitted to the outpatient clinic of our hospital. His parents reported that a “small dot” had been observed at his left cornea for 3 days. The infant was burping on the babysitter’s shoulder when this “dot” was first found. His parents and babysitter declared that no inconsolable crying or other abnormalities have occurred during the 3 days. In addition, the infant was born at full term, with no history of other illnesses, and had not been found to have rubbed his eyes.
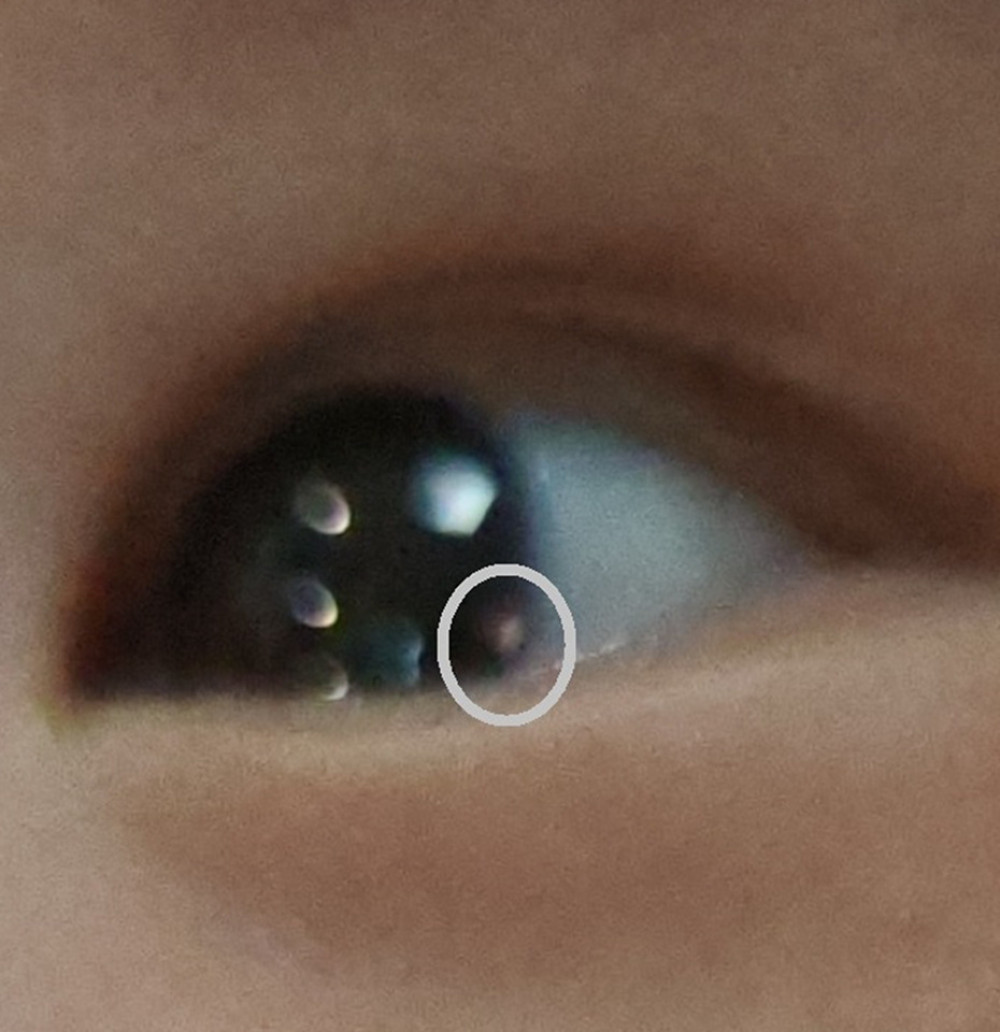
Portable slit lamp examination revealed an oval, pink, plastic foreign body in the epithelial layer of the cornea near his inferior-temporal limbus, with a diameter of approximately 0.8 mm. No evidence of bulbar redness or refractory media opacity was observed (Figure 1). The family members’ recollection suggested that the foreign body was determined to be an ornament affixed to the dress that the babysitter was wearing at the time.
With the consent of the infant’s guardian (his mother), the infant was placed on a treatment bed, and topical anesthesia was administered using 0.5% proparacaine hydrochloride eye drops (Alcon Inc), followed by CFB removal. Sedation with chloral hydrate oral solution was rejected by the guardian. Considering the infant’s limited ability to cooperate, we initially attempted to remove the foreign body by flushing it out with saline, and failed. Then, we tried CFB removal by using a sterile cotton-tipped applicator, but also encountered difficulty due to its firm adhesion to the cornea. Subsequently, we directed the assistant to stabilize the infant’s head position. Thereafter, we re-administered proparacaine hydrochloride drops to the conjunctival sac and meticulously released the foreign body from the cornea with a 1-mL needle (26 gauge) tip while the eye drops remained on the surface of the conjunctival sac and cornea. We then expeditiously removed the CFB using a sterile cotton-tipped applicator. After removal of the CFB, the infant’s ocular surface appearance showed no obvious abnormality. Topical administration of 0.3% tobramycin eye drops (Alcon) were used to prevent infection. No bulbar redness, corneal opacities, infection, or adverse effects were found during the 3-day and 1-week follow-ups. The patient’s parents were satisfied with the treatment.
Discussion
This case report demonstrates the absence of significant symptoms of a plastic CFB in a young infant, highlighting the importance of comprehensive parental care. Also, a viable and low-risk office-based approach to address the issue of CFB removal in young infants is indicated.
For many years, cases of CFB injury were classified as minor ocular trauma [8], as the condition generally did not result in severe complications if the removal procedure was performed promptly. However, if the CFB is ignored or removal is delayed, it can lead to keratitis or even endophthalmitis. Furthermore, in the case of children, particularly infants, failure to remove or delaying the removal of CFB can result in astigmatism or amblyopia, which can have a detrimental impact on their lifelong visual quality [11].
Previous case reports have described metallic CFBs in children, often presenting with pronounced symptoms such as foreign body sensation and conjunctival redness [5,7,12]. In contrast, the patient in our case presented no symptoms, suggesting the uniqueness of small plastic CFBs and the young age of occurrence. Therefore, a thorough and timely examination is critical for CFBs of materials such as plastic [4] and for young patients. Given the infant’s limited cooperation and, in this case, the parents’ refusal of medical sedation, performing a thorough slit lamp examination and fluorescein dye was challenging. Such examinations are, however, essential for most cases of CFB [2,3]. Therefore, a comprehensive clinical history obtained from parents and/or all relevant individuals regarding risk factors and exposure is of paramount importance. Also, it is important to acknowledge the significance of ruling out open-globe injuries [13], although such injuries were not observed in this case.
Despite the long-standing recognition of CFB removal as an entry-level skill [14], this procedure still poses significant challenges for infant patients due to their inability to communicate or cooperate. In the present case, the administration of sedation was declined, thereby exacerbating the inherent challenges. During the CFB removal procedure, assistants must meticulously adjust the infant’s head position, control body twisting, and if necessary, use an infant-specific lid opener to ensure complete field exposure. Ensuring proper head and eye positioning is critical for enabling the operator to successfully remove the foreign body. In our case, the operator did not attempt to extract the foreign body with a needle; rather, the needle was used to gently dislodge the CFB, thereby allowing fluid from the conjunctival sac and corneal surface to infiltrate the space between the foreign body and the cornea. This cautious approach, emphasizing safety, is particularly important in pediatric cases, especially those involving young infants.
This case report also underscores the importance of prompt recognition and identification of ocular CFBs for parents, caregivers, babysitters, and all individuals responsible for infant care. This need arises from the small size of such foreign bodies, which often escape detection. Furthermore, as observed in our case, the typical crying response to the foreign body in young infants can be absent due to their underdeveloped ability to experience significant corneal neuropathic pain. Consequently, there is a need for public education to underscore the necessity of round-the-clock care for very young infants and to promote awareness of ocular abnormalities.
Conclusions
Plastic CFBs in young infants can present without symptoms and thus can be easily ignored. Also, because CFB removal in young infants is usually challenging, this report proposes a viable and low-risk office-based approach to address the issue of CFB removal in these young patients.
References
1. Aziz MA, Rahman MA, Corneal foreign body – an occupational hazard: Mymensingh Med J, 2004; 13(2); 174-76
2. Ahmed F, House RJ, Feldman BH, Corneal abrasions and corneal foreign bodies: Prim Care, 2015; 42(3); 363-75
3. Camodeca AJ, Anderson EP, Corneal foreign body: StatPearls, 2025, Treasure Island (FL), StatPearls Publishing
4. Etheridge TJ, Jones J, Werner L, Plastic orbital foreign body: The rise of plastic and its unintended consequences: Orbit, 2024; 43(4); 511-15
5. Stepankova J, Odehnal M, Malec J, Dotrelova D, Corneal foreign bodies in children: Cesk Slov Oftalmol, 2012; 68(4); 142-45
6. Ramakrishnan T, Constantinou M, Jhanji V, Vajpayee RB, Corneal metallic foreign body injuries due to suboptimal ocular protection: Arch Environ Occup Health, 2012; 67(1); 48-50
7. Kehat R, Bonsall DJ, Recurrent corneal metallic foreign bodies in children with autism spectrum disorders: J AAPOS, 2009; 13(6); 621-22
8. Shrestha T, Parajuli S, Sharma S, Clinical profile of patients presenting with corneal foreign bodies: A cross-sectional study conducted in a tertiary hospital in Nepal: Nepal J Ophthalmol, 2022; 14(27); 59-64
9. Agrawal C, Girgis S, Sethi A, Etiological causes and epidemiological characteristics of patients with occupational corneal foreign bodies: A prospective study in a hospital-based setting in India: Indian J Ophthalmol, 2020; 68(1); 54-57
10. Xu J, Xu G, Epidemiology of corneal foreign bodies of QuanGang district in FuJian province: Chinese Journal of Practical Ophthalmology, 2009; 27(2); 186-88
11. Meek KM, Knupp C, Corneal structure and transparency: Prog Retin Eye Res, 2015; 49; 1-16
12. Ozkurt ZG, Yuksel H, Saka G, Metallic corneal foreign bodies: An occupational health hazard: Arq Bras Oftalmol, 2014; 77(2); 81-83
13. Loporchio D, Mukkamala L, Gorukanti K, Intraocular foreign bodies: A review: Surv Ophthalmol, 2016; 61(5); 582-96
14. Hamlyn BR, Hart KM, Kiely PM, Entry-level competency standards for optometry 2022: Clin Exp Optom, 2025; 108(3); 380-93
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133