26 December 2025: Articles 
Primary Well-Differentiated Neuroendocrine Tumor of the Breast: A Case Report and Literature Review
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Patient complains / malpractice, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Sanjna Sai Gudena DEF 1*, Nilesh Digvijay Kashikar E 2, Matthew Charles Wakefield E 3DOI: 10.12659/AJCR.950684
Am J Case Rep 2025; 26:e950684






Abstract
BACKGROUND: Primary breast neuroendocrine neoplasms (NENs) are extremely rare, comprising 1-5% of diagnosed breast cancers. The goal of this paper is to describe the current literature on these cancers, along with treatment options and survival data from prior studies.
CASE REPORT: A 61-year-old woman presented with a palpable lump in the breast, which upon biopsy was proven to be a primary breast neuroendocrine tumor. This was treated with breast-conserving surgery with sentinel lymph node dissection, followed by adjuvant radiation. She refused anti-estrogen therapy, and 2 years later she presented with metastatic disease, chose not to receive any additional treatment, and died. Several retrospective analyses have illustrated that breast neuroendocrine tumors have a slightly worse prognosis compared to invasive ductal carcinomas (IDCs) when stratified by stage. However, most of the studies had small sample sizes, which makes interpretation of data from these studies difficult to generalize to the overall population of breast NENs.
CONCLUSIONS: Routine testing for neuroendocrine markers could identify a larger population of neuroendocrine tumors (NETs). Currently, because of the rarity of these tumors, prospective trials are not available to study them as a distinct entity to evaluate and optimize treatments. Reports indicate that these tumors have overall inferior survival compared to IDCs. Further studies are needed to evaluate this rare entity to improve patient outcomes.
Keywords: neuroendocrine tumors, Breast Neoplasms, Case Reports, Humans, Female, Middle Aged, Mastectomy, Segmental, Sentinel Lymph Node Biopsy, Fatal Outcome
Introduction
PATHOLOGICAL DEFINITION OF BREAST NEUROENDOCRINE NEOPLASMS (NEN):
Previously, the WHO classification of breast neuroendocrine carcinomas required more than 50% of cells to have neuroendocrine features, but this has been changed over the years. In 2019, the WHO classified NENs of the breast, like other organs, into well-differentiated neuroendocrine tumors (NETs), highly aggressive neuroendocrine carcinomas (NECs), and invasive breast cancers of no special type (IBCs-NST) with neuroendocrine differentiation [4].
There are several markers for identification of neuroendocrine lineage, including synaptophysin, chromogranin A, somatostatin receptors, and INSM1. Other immunohistochemical markers can identify the primary source, which include estrogen receptors, progesterone receptors, HER-2 neu receptors, and cytokeratins [5].
Case Report
TREATMENT SUMMARY:
The patient underwent breast-conserving surgery and sentinel lymph node biopsy. Final pathology revealed a breast primary neuroendocrine tumor measuring 2.8 cm with clear margins, and 2 lymph nodes from the left axilla were negative for malignancy. After discussing the risks and benefits of chemotherapy, the decision was made to forego chemotherapy. Subsequently, she underwent adjuvant radiation therapy, receiving 42 Gray in 16 fractions and 8 Gray boost over 4 fractions. She was prescribed adjuvant anti-estrogen therapy with anastrozole with the planned treatment duration of 5–7 years.
After a few months of anti-estrogen therapy, she discontinued it because of adverse effects, primarily hot flashes and joint stiffness, and was lost to follow-up until she presented to the hospital 2 years later with low back pain and severe hypercalcemia (serum calcium level >15 mg/dL). A workup revealed a 5.8-cm right upper-lobe lung mass, pathologic mediastinal adenopathy, and multifocal osseous metastatic disease throughout the ribs, spine, and scapula (Figure 6). Her back pain was the result of a pathologic compression fracture of the T7 vertebral body with extraosseous extension (Figure 7). Bronchoscopy biopsy and immunohistochemical (IHC) stains revealed malignant cells that were GATA3-positive and TTF-1/p40-negative (Figure 8A, 8B). This profile was most consistent with a breast carcinoma metastasis, similar to her earlier diagnosis of breast NET. She declined all further therapy, entered hospice care, and died 1 month later.
Discussion
Several retrospective analyses of breast NEN have been conducted over the past 2 decades. Most studies are hampered by small sample sizes and comparison with historical controls, making it difficult to generalize the data to the wider population of breast NENs (Table 1). The largest such retrospective analysis of the National Cancer Database was published in
Earlier studies also appear to show that breast NETs have worse outcomes than IDCs. This was studied by Wang et al in a retrospective analysis of the Surveillance, Epidemiology, and End Results (SEER) database from 2003 to 2009 with a sample size of 142. Similarly, estrogen receptor- and progesterone-negative tumors were more often seen in the neuroendocrine cohort, and 5-year overall survival was 53.6% for NET versus 79.8% for invasive mammary carcinomas (IMC). Once again, at each stage, the overall survival was inferior in the neuroendocrine cohort [6].
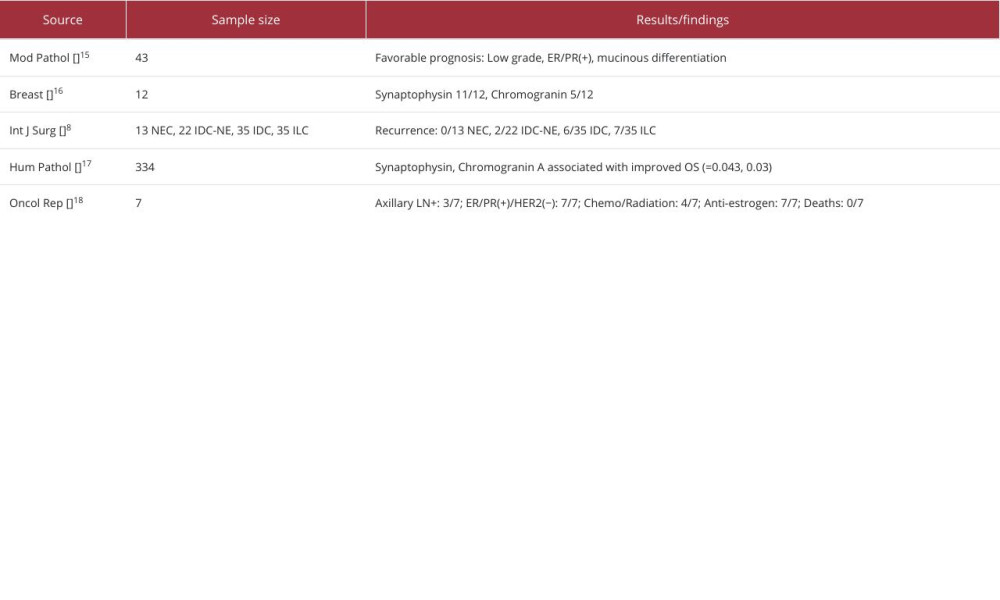
Other studies are summarized in Table 2, but because of small sample sizes, definitive conclusions are difficult. However, they are worthy of discussion, given the relative paucity of data on these cancers. Sapino et al analyzed prognostic markers for NECs and found that low-grade ER-/PR-positive expression and mucinous differentiation are associated with a favorable prognosis [7].
Rovera et al evaluated NETs (defined as >50% positivity for NE markers) and compared them to ductal carcinomas with <50% NE markers. They did not find NETs have a worse prognosis compared to the IDCs with minor neuroendocrine marker positivity. They also compared NEC to IDC and ILC, finding that patients with NEC did not have cancer recurrences, showing that NECs were less aggressive. This has not been shown in any other studies and hence is an outlier. The small sample size makes it difficult to draw definitive conclusions [8].
The overall incidence and prevalence of all neuroendocrine tumors have been steadily growing, owing to better diagnostic testing and early stages of diagnosis due to better screening techniques. Simultaneously, survival of all neuroendocrine tumors has also been improving, especially because of improved systemic treatments and early detection. However, there is very little data on breast neuroendocrine cancers in this study of the SEER database from 2009 to 2012 [6].
Oncotype Dx and Mammaprint molecular testing have become essential tools for risk stratification and determination of chemotherapy benefit for ER-positive and HER-2 negative breast cancers. Neither study identified NEC in their subset analysis to enable use of these tools for risk stratification. The role of chemotherapy in these cancers is unclear due to a lack of relevant data from these studies [9,10].
A significant aspect of our case was the early discontinuation of anti-estrogen therapy, which could have affected the relapse and mortality of our patient. A meta-analysis published in 2023 by Eliassen et al analyzed non-adherence or early discontinuation (non-persistent) of anti-estrogen therapy in estrogen receptor-positive breast cancer patients. Out of 10 studies, 7 showed significantly poorer event-free survival for the non-adherent or non-persistent patient groups, with hazard ratios (HRs) ranging from 1.39 (95% CI, 1.07 to 1.53) to 2.44 (95% CI, 1.89 to 3.14). Seven out of 10 studies also demonstrated significantly reduced overall survival in the groups with non-adherence and non-persistence, with HRs ranging from 1.26 (95% CI, 1.11 to 1.43) to 2.18 (95% CI, 1.99 to 2.39) [11].
CDK 4/6 inhibitors like abemaciclib have been approved for the adjuvant treatment of hormone receptor-positive, HER2-negative, node-positive, early breast cancer at a high risk of recurrence based on the MONARCH-E clinical trial [12,13]. Ribociclib has also received approval for use in Stage 2 and 3 ER-positive breast cancers with high-risk features [13]. However, neither study had any data on neuroendocrine differentiation. A case report published by Zouki et al in a patient with metastatic breast NEC demonstrated a positive response to endocrine therapy with palbociclib and triptorelin [12,14]. Therefore, the clinical benefit of these novel agents in the treatment of NENs must be further investigated.
Conclusions
Our case illustrates a typical presentation of a neuroendocrine tumor of the breast, most of which are estrogen- and progesterone receptor-positive and HER2-negative. The treatment approach is similar to that of invasive ductal carcinoma, with a combination of therapeutic options that include surgery, chemotherapy, radiation, and anti-estrogen therapies. Because of a lack of prospective randomized control trials, whether this approach is adequate or excessive cannot be determined.
The role of novel CDK 4/6 inhibitors in the adjuvant therapy of estrogen receptor-positive breast NEN has not been established. There have not been any randomized clinical trials to compare outcomes with and without chemotherapy. Molecular analysis using Oncotype DX or Mammaprint is also lacking to determine the risk of recurrence and to understand the benefit of systemic chemotherapy. Universal testing for neuroendocrine markers could identify a larger subset of breast neuroendocrine tumors that could be better studied using prospective randomized controlled clinical trials.
Figures
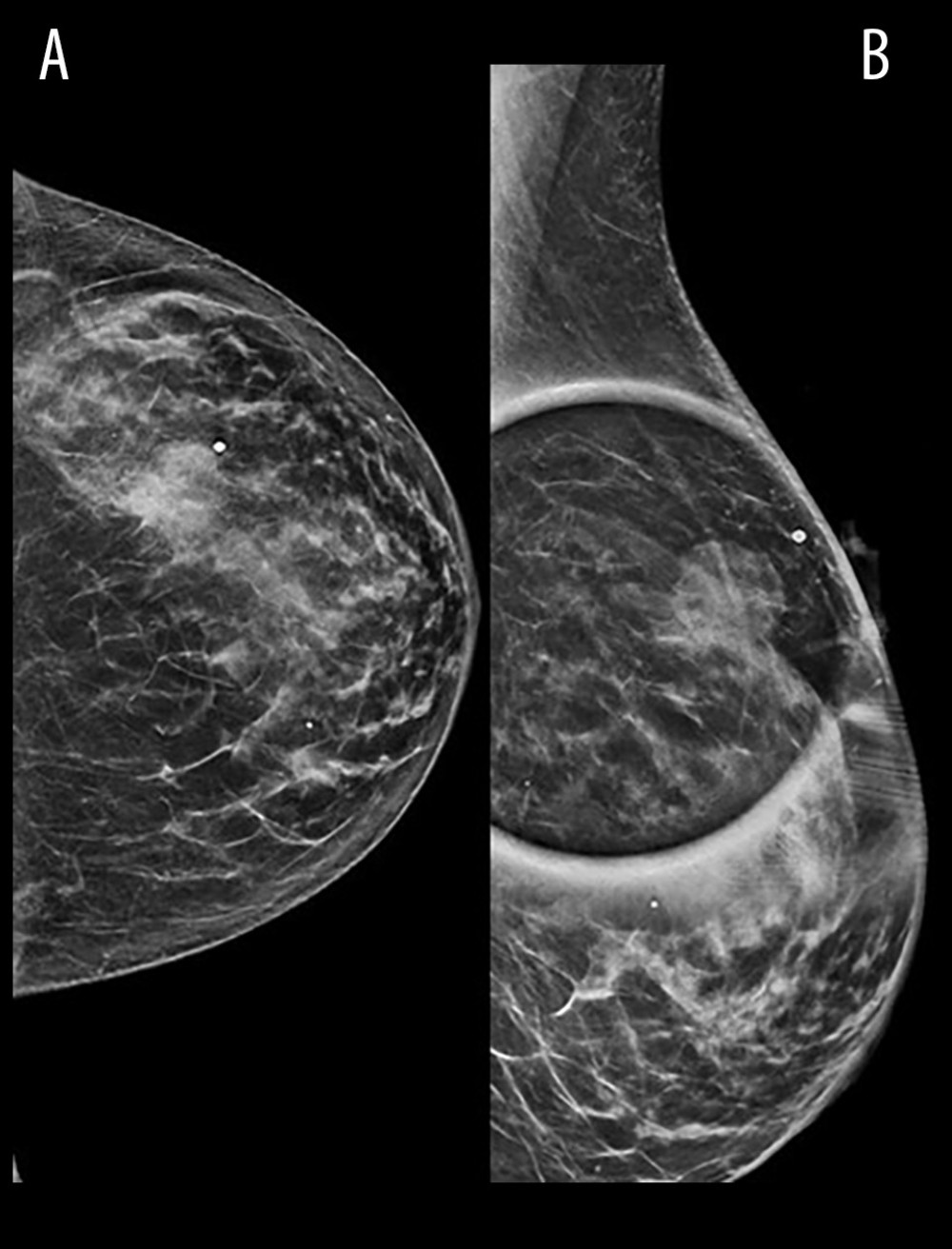 Figure 1. (A) Mammogram revealing a 2.6-cm mass in the left breast upper outer quadrant. (B) CC view confirming the breast mass.
Figure 1. (A) Mammogram revealing a 2.6-cm mass in the left breast upper outer quadrant. (B) CC view confirming the breast mass. 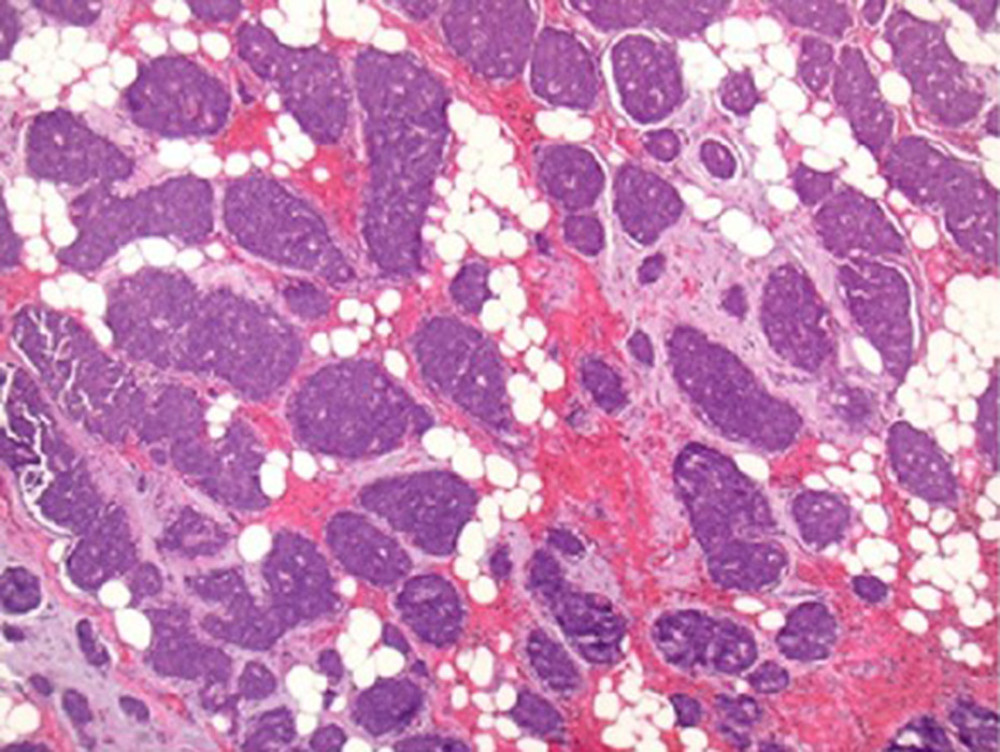 Figure 2. Low-magnification view (40×) of the tumor with H&E stain, showing tumor cells arranged in tight organoid nests with delicate intervening fibrovascular stroma. Almost the entire tumor shows the same pattern.
Figure 2. Low-magnification view (40×) of the tumor with H&E stain, showing tumor cells arranged in tight organoid nests with delicate intervening fibrovascular stroma. Almost the entire tumor shows the same pattern. 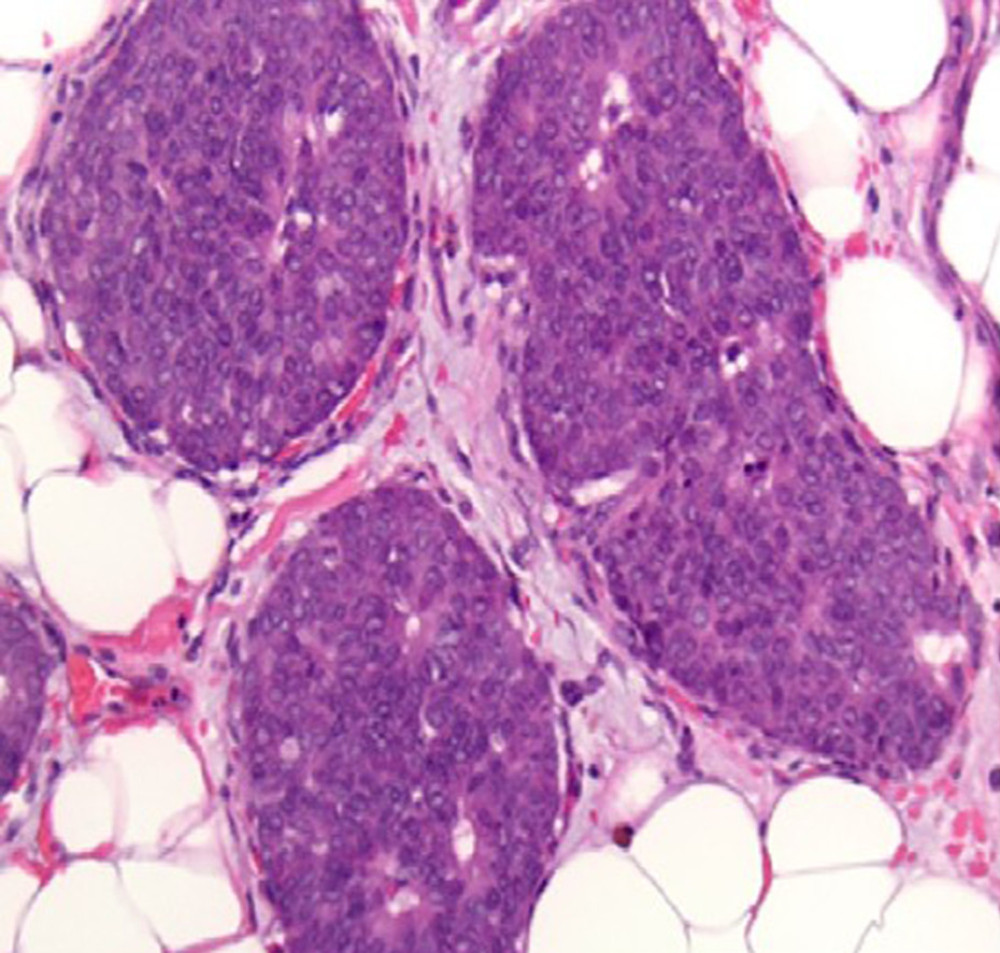 Figure 3. At a higher magnification (200×), the tumor cells show many typical features of neuroendocrine morphology. The tumor cells are polygonal with granular eosinophilic cytoplasm. The classical salt-and-pepper stippled chromatin is visible in a minority of tumor cells. Neuroendocrine tumors of the breast in general, as also seen in this case, tend to show a lower Nottingham nuclear grade of 1 or 2 out of 3.
Figure 3. At a higher magnification (200×), the tumor cells show many typical features of neuroendocrine morphology. The tumor cells are polygonal with granular eosinophilic cytoplasm. The classical salt-and-pepper stippled chromatin is visible in a minority of tumor cells. Neuroendocrine tumors of the breast in general, as also seen in this case, tend to show a lower Nottingham nuclear grade of 1 or 2 out of 3. 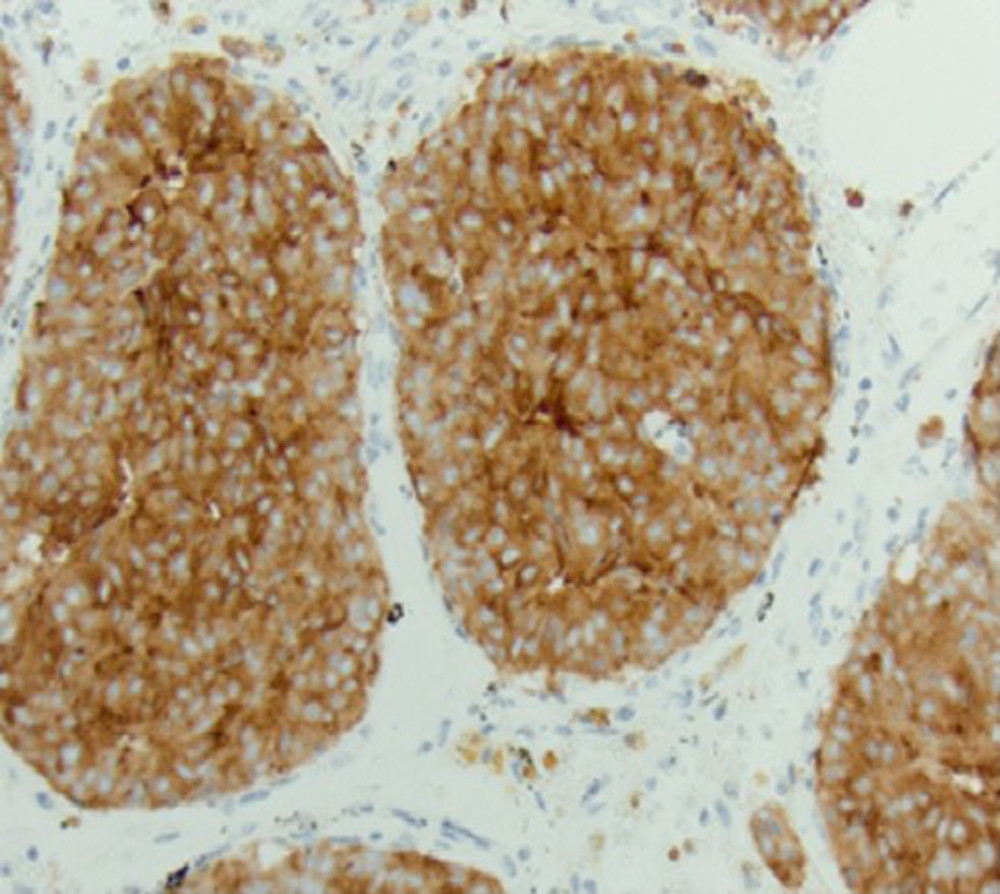 Figure 4. Immunohistochemical stain for synaptophysin, a typical marker for neuroendocrine differentiation, displays cytoplasmic labeling within the tumor cells, confirming the neuroendocrine nature of the tumor.
Figure 4. Immunohistochemical stain for synaptophysin, a typical marker for neuroendocrine differentiation, displays cytoplasmic labeling within the tumor cells, confirming the neuroendocrine nature of the tumor. 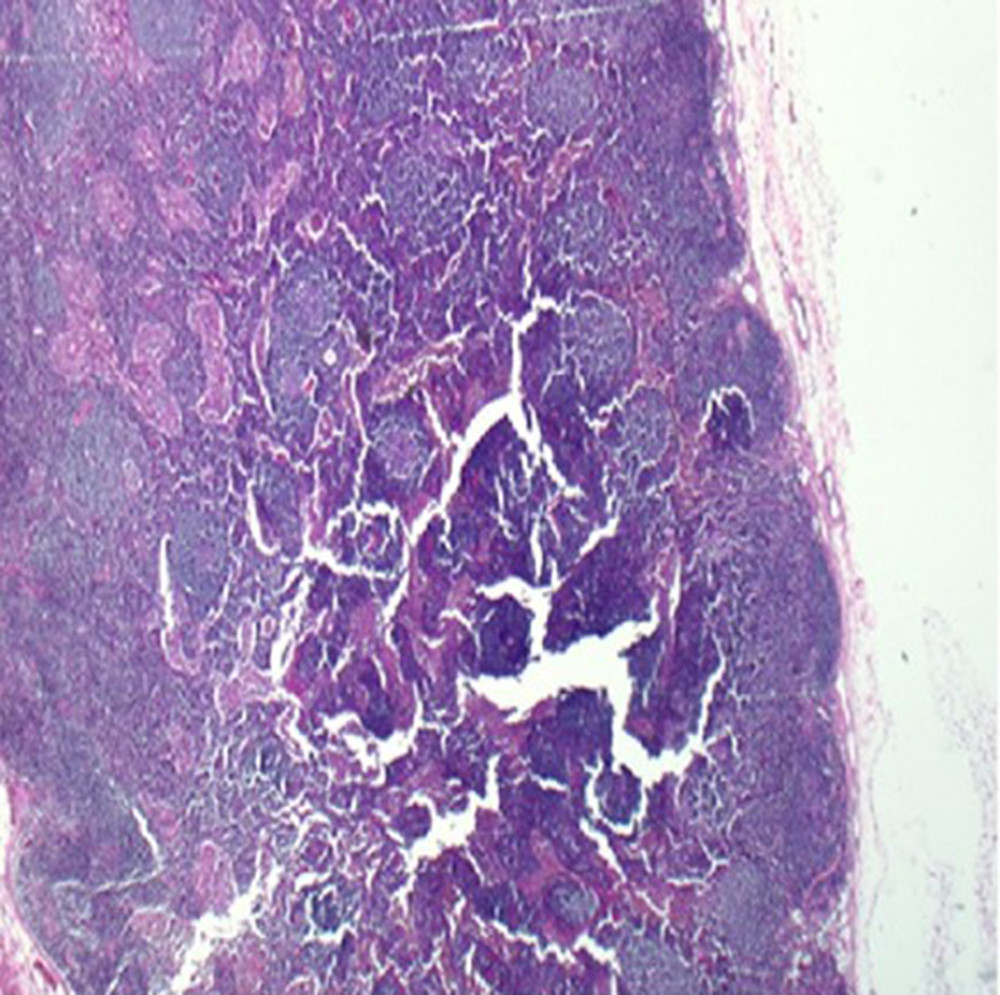 Figure 5. A representative micrograph from one of the lymph nodes showing normal lymph node architecture with lymphoid follicles and sinusoids, without any evidence of metastatic tumor.
Figure 5. A representative micrograph from one of the lymph nodes showing normal lymph node architecture with lymphoid follicles and sinusoids, without any evidence of metastatic tumor. 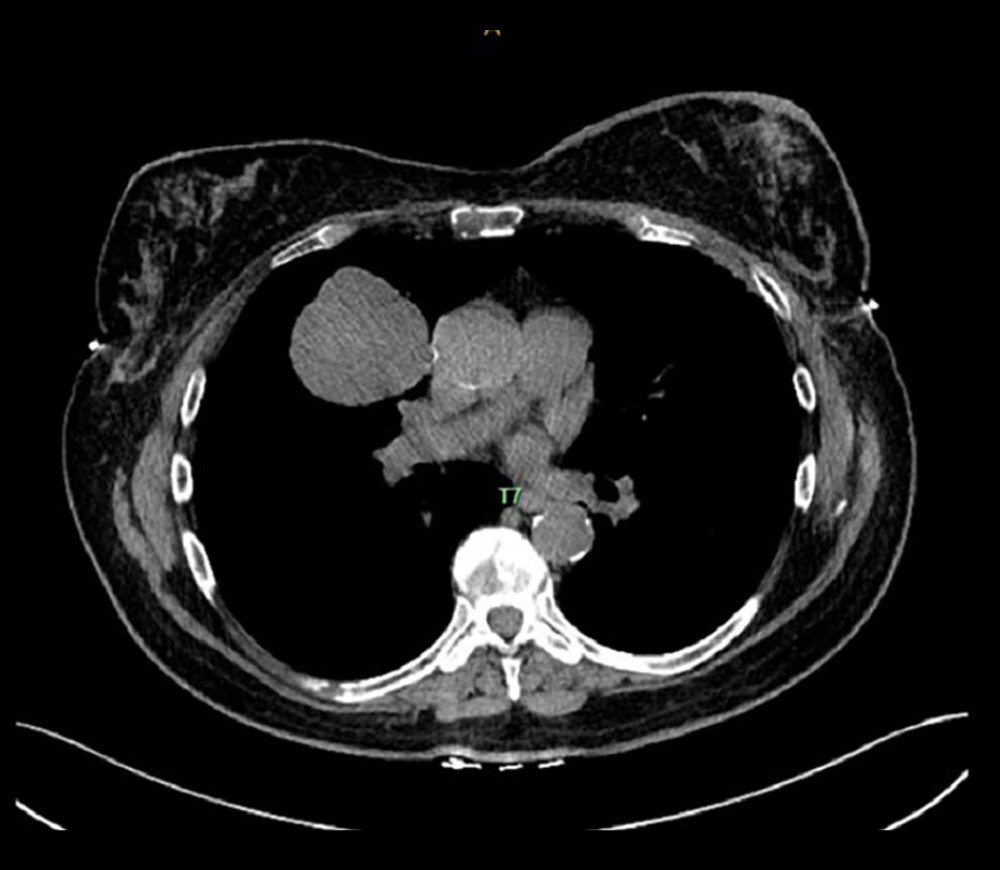 Figure 6. Computed tomography showing the right upper-lobe lung mass and mediastinal lymphadenopathy.
Figure 6. Computed tomography showing the right upper-lobe lung mass and mediastinal lymphadenopathy. 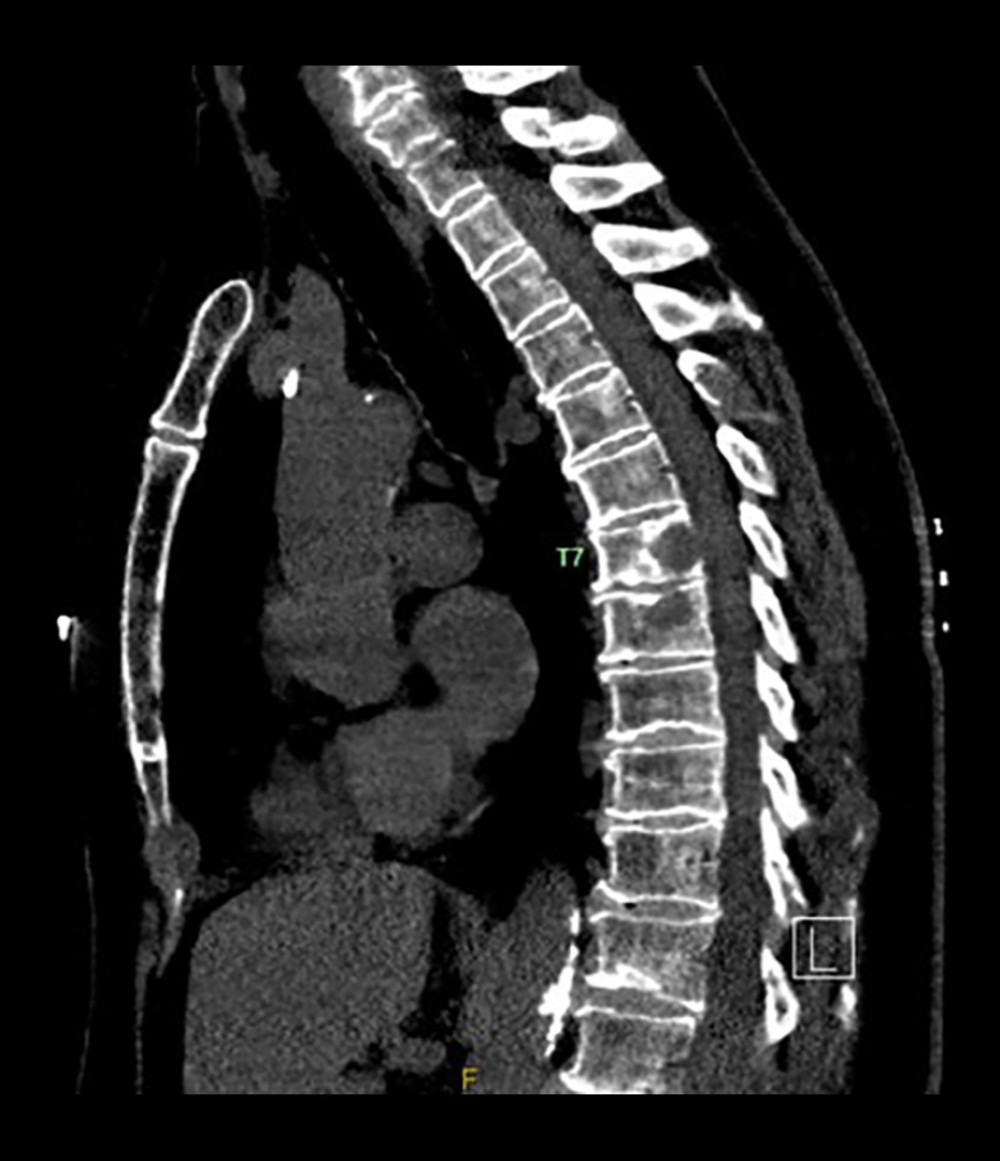 Figure 7. Computed tomography of the thoracic spine showing a T7 vertebral compression fracture.
Figure 7. Computed tomography of the thoracic spine showing a T7 vertebral compression fracture. 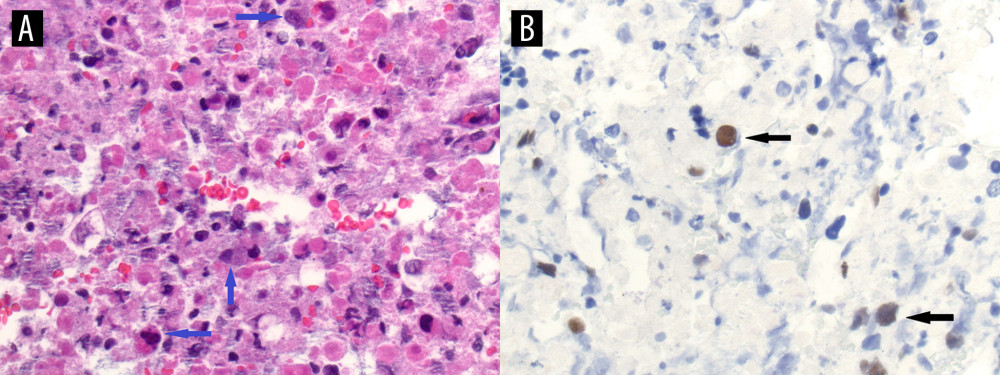 Figure 8. Lung involvement by metastatic breast carcinoma. (A) High-power magnification image of the H&E-stained fine-needle aspirate from the lung lesion appears to be predominantly necrotic with an admixture of inflammatory cells, macrophages, and a few probable metastatic malignant cells (blue arrows). (B) Immunohistochemical stain for a breast marker, GATA3, was performed. The stain labeled rare, scattered, malignant-appearing cells (black arrows), confirming the presence of metastatic breast carcinoma to the lung.
Figure 8. Lung involvement by metastatic breast carcinoma. (A) High-power magnification image of the H&E-stained fine-needle aspirate from the lung lesion appears to be predominantly necrotic with an admixture of inflammatory cells, macrophages, and a few probable metastatic malignant cells (blue arrows). (B) Immunohistochemical stain for a breast marker, GATA3, was performed. The stain labeled rare, scattered, malignant-appearing cells (black arrows), confirming the presence of metastatic breast carcinoma to the lung. 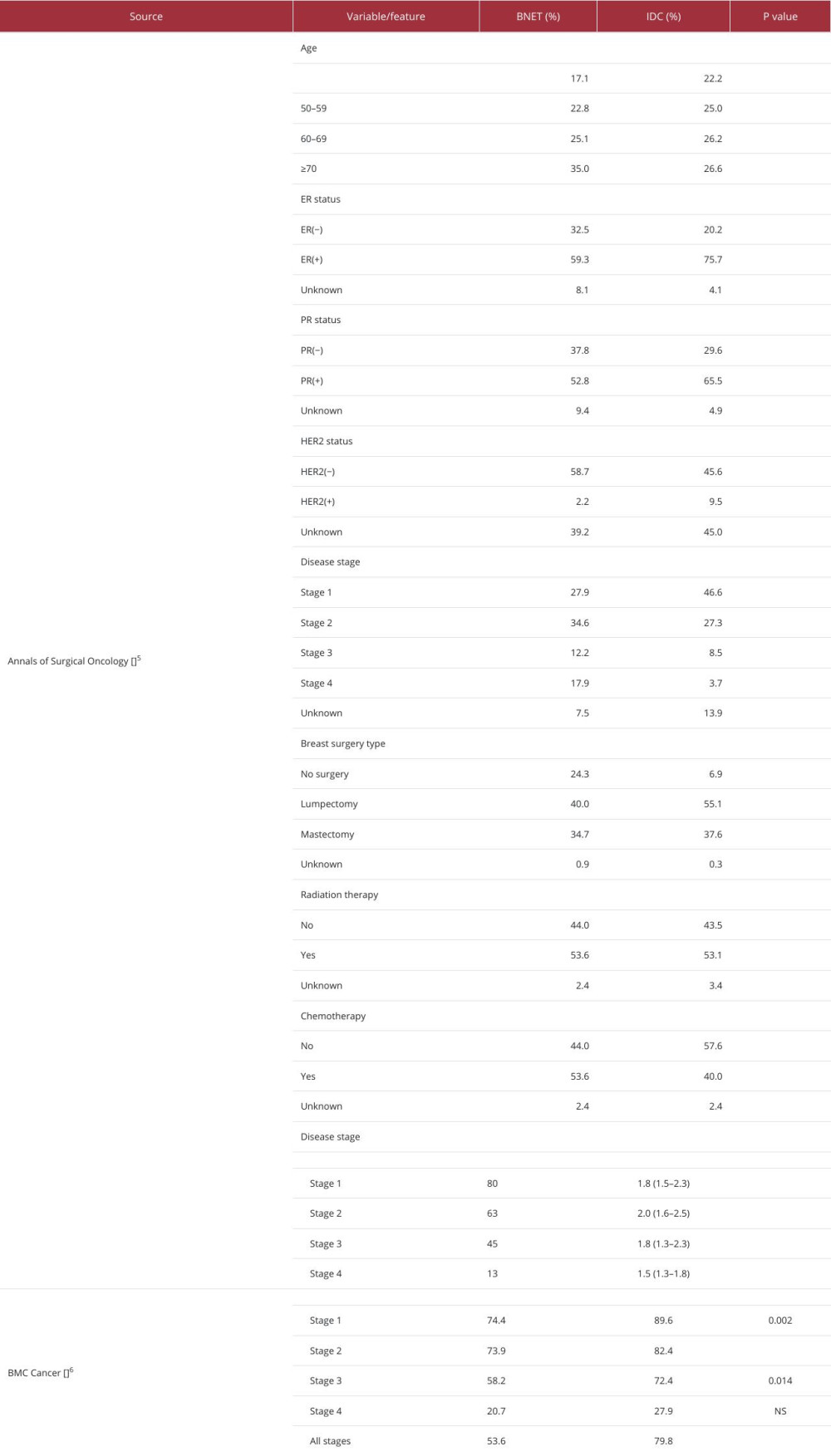
References
1. Dasari A, Shen C, Halperin D, Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States: JAMA Oncol, 2017; 3(10); 1335-42
2. Wei B, Ding T, Xing Y, Invasive neuroendocrine carcinoma of the breast: A distinctive subtype of aggressive mammary carcinoma: Cancer, 2010; 116(19); 4463-73
3. Bogina G, Munari E, Brunelli M, Neuroendocrine differentiation in breast carcinoma: clinicopathological features and outcome: Histopathology, 2016; 68(3); 422-32
4. Rindi G, Mete O, Uccella S, Overview of the 2022 WHO Classification of neuroendocrine neoplasms: Endocr Pathol, 2022; 33(1); 115-54
5. Martinez EO, Jorns JM, Kong AL, Primary breast neuroendocrine tumors: An analysis of the National Cancer Database: Ann Surg Oncol, 2022; 29(10); 6339-46
6. Wang J, Wei B, Albarracin CT, Hu J, Invasive neuroendocrine carcinoma of the breast: A population-based study from the surveillance, epidemiology and end results (SEER) database: BMC Cancer, 2014; 14; 147
7. Sapino A, Papotti M, Righi L, Clinical significance of neuroendocrine carcinoma of the breast: Ann Oncol, 2001; 12(Suppl 2); S115-17
8. Rovera F, Masciocchi P, Coglitore A, Neuroendocrine carcinomas of the breast: Int J Surg, 2008; 6(Suppl 1); S113-15
9. Cardoso F, van’t Veer LJ, Bogaerts J, 70-gene signature as an aid to treatment decisions in early-stage breast cancer: N Engl J Med, 2016; 375(8); 717-29
10. Sparano JA, Gray RJ, Makower DF, Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer: N Engl J Med, 2018; 379(2); 111-21
11. Eliassen FM, Blafjelldal V, Helland T, Importance of endocrine treatment adherence and persistence in breast cancer survivorship: A systematic review: BMC Cancer, 2023; 23(1); 625
12. Johnston SRD, Andre V, Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk, early breast cancer – Authors’ reply: Lancet Oncol, 2023; 24(3); e104
13. Slamon D, Yardley DA, Hortobagyi G, Ribociclib plus endocrine therapy in early breast cancer. Reply: N Engl J Med, 2024; 390(23); 2221-22
14. Zouki DN, Kardara VE, Ioannou S, CDK4/6 and aromatase inhibitors as first-line treatment in metastatic high-grade neuroendocrine carcinoma of the breast: A case report: Clin Case Rep, 2024; 12(7); e9180
15. Lavigne M, Menet E, Tille JC, Comprehensive clinical and molecular analyses of neuroendocrine carcinomas of the breast: Mod Pathol, 2018; 31(1); 68-82
16. Zekioglu O, Erhan Y, Ciris M, Bayramoglu H, Neuroendocrine differentiated carcinomas of the breast: A distinct entity: Breast, 2003; 12(4); 251-57
17. Makretsov N, Gilks CB, Coldman AJ, Tissue microarray analysis of neuroendocrine differentiation and its prognostic significance in breast cancer: Hum Pathol, 2003; 34(10); 1001-8
18. Lopez-Bonet E, Alonso-Ruano M, Barraza G, Solid neuroendocrine breast carcinomas: incidence, clinico-pathological features and immunohistochemical profiling: Oncol Rep, 2008; 20(6); 1369-74
Figures
Figure 1. (A) Mammogram revealing a 2.6-cm mass in the left breast upper outer quadrant. (B) CC view confirming the breast mass.Figure 2. Low-magnification view (40×) of the tumor with H&E stain, showing tumor cells arranged in tight organoid nests with delicate intervening fibrovascular stroma. Almost the entire tumor shows the same pattern.Figure 3. At a higher magnification (200×), the tumor cells show many typical features of neuroendocrine morphology. The tumor cells are polygonal with granular eosinophilic cytoplasm. The classical salt-and-pepper stippled chromatin is visible in a minority of tumor cells. Neuroendocrine tumors of the breast in general, as also seen in this case, tend to show a lower Nottingham nuclear grade of 1 or 2 out of 3.Figure 4. Immunohistochemical stain for synaptophysin, a typical marker for neuroendocrine differentiation, displays cytoplasmic labeling within the tumor cells, confirming the neuroendocrine nature of the tumor.Figure 5. A representative micrograph from one of the lymph nodes showing normal lymph node architecture with lymphoid follicles and sinusoids, without any evidence of metastatic tumor.Figure 6. Computed tomography showing the right upper-lobe lung mass and mediastinal lymphadenopathy.Figure 7. Computed tomography of the thoracic spine showing a T7 vertebral compression fracture.Figure 8. Lung involvement by metastatic breast carcinoma. (A) High-power magnification image of the H&E-stained fine-needle aspirate from the lung lesion appears to be predominantly necrotic with an admixture of inflammatory cells, macrophages, and a few probable metastatic malignant cells (blue arrows). (B) Immunohistochemical stain for a breast marker, GATA3, was performed. The stain labeled rare, scattered, malignant-appearing cells (black arrows), confirming the presence of metastatic breast carcinoma to the lung. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133