28 December 2025: Articles 
Thoracic Multiple-Gunshot Suicide in a Homicide–Suicide Incident: An Unusual Case
Clinical situation which can not be reproduced for ethical reasons, Rare coexistence of disease or pathology
Yishan Lyu DEF 1, Lydia M. Sadlowski ACDEF 2, Alexander Megremis DE 3, Zhuo Wang AG 4*DOI: 10.12659/AJCR.950699
Am J Case Rep 2025; 26:e950699






Abstract
BACKGROUND: Suicide involving multiple gunshot wounds is rare, representing a small subset of firearm-related suicides, and presents significant challenges in distinguishing it from homicide. This difficulty is amplified in homicide–suicide scenarios, where accurate classification has major medico–legal implications. Thoracic wounds, particularly those involving the heart, are typically rapidly incapacitating, making multiple self-inflicted injuries unusual.
CASE REPORT: We present a case of a 43-year-old man who fatally shot his spouse, injured his stepdaughter, and then sustained 3 gunshot wounds to the chest from a semiautomatic handgun. Autopsy revealed injuries to the heart and left lung with corresponding exit wounds on the left flank and back. No soot, stippling, or muzzle imprint was observed externally, likely due to thick clothing. Ballistic testing detected vaporous lead residues on the garment at each entrance site, while histologic analysis confirmed subcutaneous gunpowder deposition with vital reaction. Body-worn camera footage documented all 3 self-inflicted gunshots occurring within 1 second, confirming a continuous firing sequence without third-party involvement. Toxicology identified a blood alcohol concentration of 0.136%, which may have contributed to disinhibition and impulsivity.
CONCLUSIONS: This case demonstrates the value of integrating autopsy, histology, ballistic testing, toxicology, and digital forensic evidence in differentiating suicide from homicide in complex cases. Body-worn camera footage provided unique temporal and contextual evidence, confirming the plausibility of rapid, multiple self-inflicted gunshot wounds. Forensic practitioners should account for the potential masking effects of clothing on residue patterns and use modern investigative tools to enhance reconstruction accuracy and support definitive medico–legal conclusions.
Keywords: Gun Violence, Homicide, Suicide, Humans, Male, adult, Wounds, Gunshot, Suicide, Completed, Thoracic Injuries, Forensic Ballistics
Introduction
Death by suicide due to multiple gunshot wounds is rare, as each wound can lead to severe disability or death. Forensic pathologists must, therefore, be thorough and meticulous in determining the cause of death as suicide in cases where the victim has multiple lethal gunshot wounds [1,2]. We present a case of death by suicide due to multiple gunshots to the chest in a homicide–suicide incident. Determining the manner of death required a meticulous investigation that integrated postmortem, ballistic, and scene analyses. Beyond its forensic value, the case also reflects a well-documented pattern of spousal homicide–suicide [3] and highlights an emerging regional concern, as Jasper County, IN has shown a steady increase in total deaths between 2018 and 2022 [4].
Case Report
A 43-year-old male victim fired 2 fatal gunshots into his wife and 1 nonfatal gunshot into his stepdaughter before turning the firearm on himself. He was found with 3 gunshot wounds in the chest from the same firearm.
The autopsy showed 3 entrance wounds on the precordial area, with injury to the heart and left lung followed by 3 exit wounds on the left flank and back (Figures 1, 2). A non-perforating laceration (3.0 cm long, 0.4 cm deep) was observed on the anterior aspect of the left ventricle of the heart, associated with the medial entrance wound. The superior and inferior entrance wounds both traversed the lower lobe of the left lung, superior and inferior portions, respectively, producing through-and-through injuries with significant pulmonary hemorrhage. Approximately 1000 mL of blood was present in the left pleural cavity, although the exact blood loss could not be estimated due to prior chest tube placement. The aorta and major great vessels were intact.
Layer-by-layer examination revealed that all 3 bullet channels were parallel, following a consistent trajectory from right to left, front to back, and slightly downward. The trajectory is consistent with self-infliction while holding the weapon in the right hand. Because all 3 bullets were discharged within seconds, the order of the shots could not be reconstructed. In addition, each wound was individually fatal due to massive bleeding and combined injury to the heart and lung, leading to rapid exsanguination and cardiopulmonary failure.
Additionally, no visible muzzling imprint, soot, or gunpowder stippling was observed on the entrance wounds. Further ballistic examination detected vaporous lead residue on the 3 defects of his thick clothing, which matched each of the wound entrances. Microscopic examination of the skin also showed sparse gunpowder pigments in the subcutaneous soft tissue along the wound tract.
Analysis of a bodycam record confirmed the very short interval between each gunshot (<1 second, especially between #3 and #4), indicating continuous shooting from an automatic handgun used by only 1 perpetrator.
Discussion
The differentiation between suicide and homicide in the context of multiple gunshot wounds is one of the most challenging aspects of forensic pathology. Recognition of the anatomical location of entry and exit wounds is essential in establishing not only the trajectory and weapon range but also the plausibility of self-infliction. The present case, involving 3 gunshot wounds to the chest, aligns with a rare subset of suicides involving multiple, potentially fatal injuries. In the present case, detailed autopsy findings provided key insight into the internal trajectories and organ injuries, clarifying both the physiological mechanism and plausibility of self-infliction. The literature reports the incidence of multiple gunshot suicides ranging from 0% to 5%, with a notable male predominance [2,5]. Thoracic gunshot wounds, particularly those affecting the heart, are associated with rapid incapacitation.
The autopsy revealed that 2 gunshots traversed the lower lobe of the left lung, while 1 caused a non-perforating laceration on the anterior wall of the left ventricle. These findings explain the rapid internal hemorrhage and collapse of cardiopulmonary function that led to death by exsanguination. The intact aorta and great vessels ruled out immediate circulatory arrest, while the 3 parallel wound channels, right to left, front to back, and slightly downward, supported self-infliction. As described in previous reports [6,7], the average time to unconsciousness after cardiac injury is 5 to 15 seconds, which aligns with the brief survivability needed to fire multiple shots in rapid succession. This is further supported by the bodycam footage, which recorded the duration between #3 and #4 shots along with all last 3 shots within a 1-second interval, indicating continuous firing from a semiautomatic weapon without interspersed actions that would suggest third-party involvement.
These findings complemented the autopsy results, which already demonstrated the trajectories and organ injuries consistent with close-range discharge. Histopathologic examination of skin samples along the wound tracks revealed gunpowder particles and coagulative necrosis consistent with vital reactions, reinforcing the presence of close-range, self-inflicted wounds (Figures 3, 4). Despite the absence of soot or stippling on the skin surface, likely due to the presence of thick clothing, ballistic examination showed vaporous lead residues on the clothing, aligning with findings by clothing-mediated wound characteristics [8].
From a behavioral standpoint, this case also reflects a classical pattern of homicide–suicide, with the perpetrator first inflicting lethal and non-lethal injuries on others before turning the weapon on himself. Prior research has outlined the psychological and situational dynamics of such incidents, often characterized by domestic strife or possessive ideation [3]. The blood alcohol concentration of 0.136% may have contributed to disinhibition or impulsivity, emphasizing the influence of alcohol on judgment and motor coordination in forensic toxicology [9,10].
Although bodycam footage provided valuable corroboration of the short firing interval, it primarily served to confirm conclusions already supported by the autopsy. The temporal evidence was consistent with, but not essential to, determining the manner of death. This underscores that while digital evidence can enhance scene reconstruction, traditional postmortem examination remains decisive.
In conclusion, the autopsy was central in determining the manner and cause of death, clarifying the internal injuries, trajectories, and mechanisms of exsanguination. The integration of histologic, toxicologic, ballistic, and digital evidence further reinforced these findings, all pointing to suicide as the manner of death. This case highlights the importance of a multidisciplinary forensic approach, with the autopsy as the foundation for resolving complex firearm deaths.
Conclusions
The decisive evidence for determining the manner of death in this case came from the autopsy. Layer-by-layer examination demonstrated 3 parallel trajectories traversing the heart and lungs, consistent with close-range self-infliction. Histopathologic findings of vital reactions along the wound tracts confirmed that all injuries were sustained during life, while the intact aorta and great vessels excluded alternative mechanisms of sudden death. These observations alone were sufficient to establish suicide as the manner of death and exsanguination due to multiple gunshot wounds to the chest as the cause of death.
Digital evidence from the bodycam provided temporal corroboration but was not indispensable to this conclusion. Even without it, the autopsy, ballistic, and histologic findings independently ruled out third-party involvement. This case reinforces that, despite advances in digital forensics, the traditional postmortem examination remains the cornerstone for distinguishing suicide from homicide in complex firearm deaths.
Figures
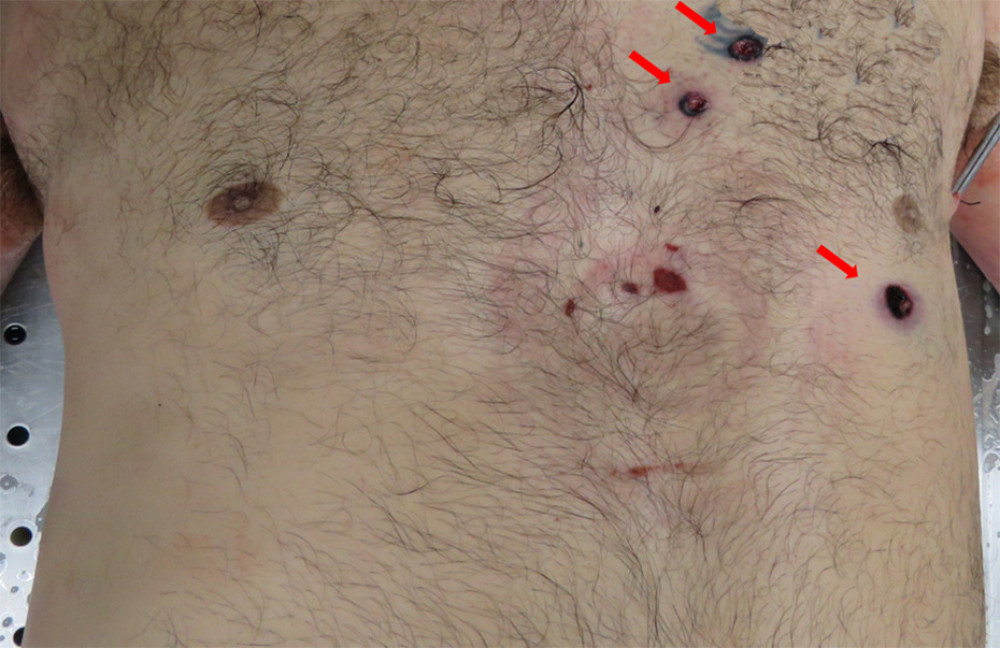 Figure 1. Anterior chest showing 3 entrance gunshot wounds clustered in the precordial region. Arrows denote wound sites. No soot or stippling visible externally. No visible soot or gunpowder stippling around wounds. Note the medical artifacts caused by a LUCAS device used for chest compressions.
Figure 1. Anterior chest showing 3 entrance gunshot wounds clustered in the precordial region. Arrows denote wound sites. No soot or stippling visible externally. No visible soot or gunpowder stippling around wounds. Note the medical artifacts caused by a LUCAS device used for chest compressions. 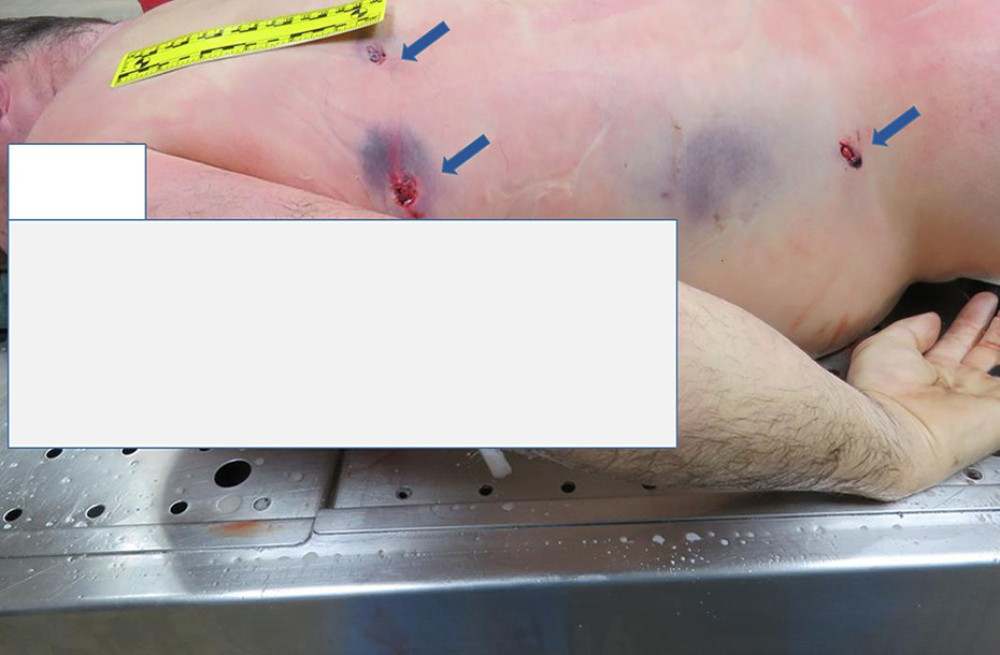 Figure 2. Three exit gunshot wounds on the left side of the back and left flank region (blue arrow) associated with 3 entrance wounds on the chest. The margins showed lacerated features.
Figure 2. Three exit gunshot wounds on the left side of the back and left flank region (blue arrow) associated with 3 entrance wounds on the chest. The margins showed lacerated features. 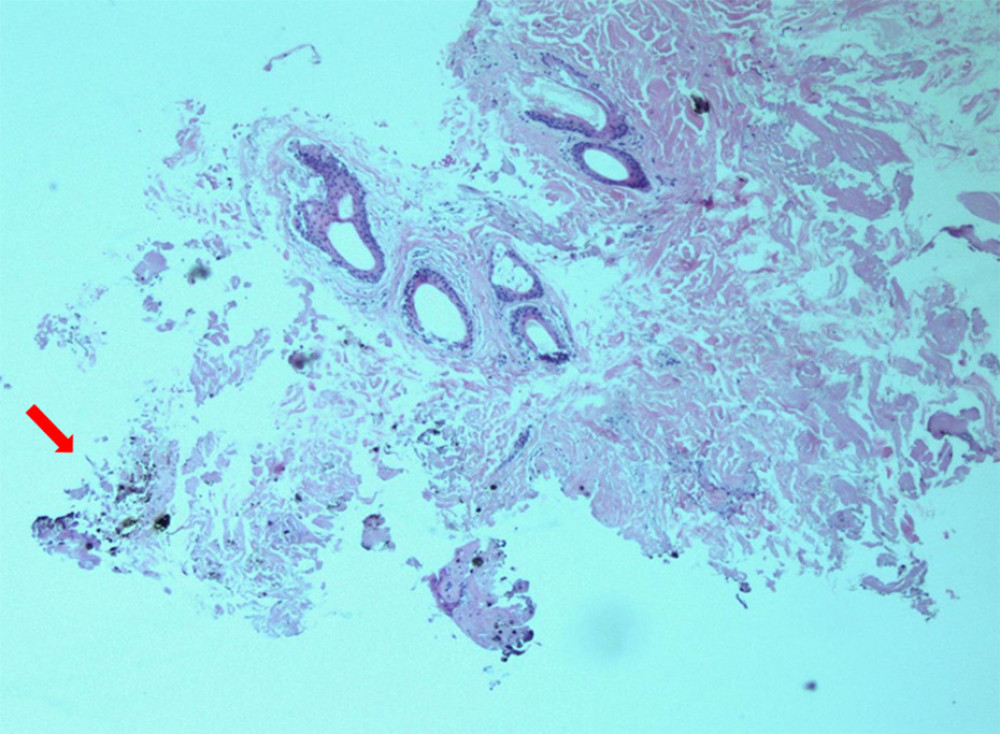 Figure 3. Histological section (H&E stain, 40× magnification) of subcutaneous tissue demonstrating sparse embedded gunpowder particles along the wound tract, consistent with close-range discharge. Disruption of the subcutaneous tissue, coagulation necrosis, and gunpowder particles deposit.
Figure 3. Histological section (H&E stain, 40× magnification) of subcutaneous tissue demonstrating sparse embedded gunpowder particles along the wound tract, consistent with close-range discharge. Disruption of the subcutaneous tissue, coagulation necrosis, and gunpowder particles deposit. 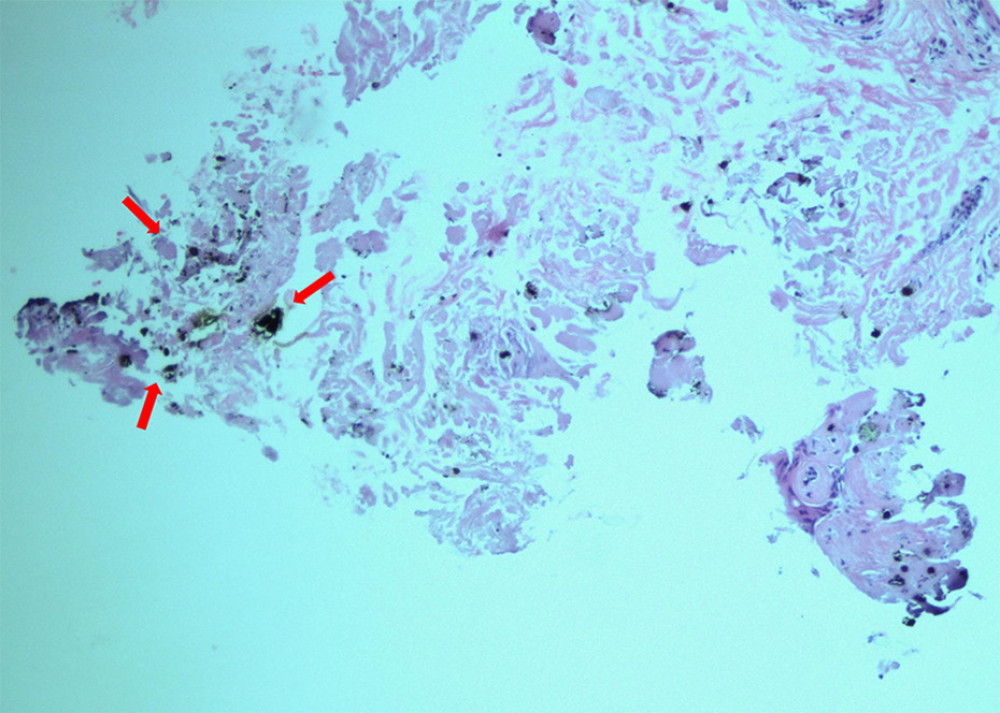 Figure 4. Histological section of subcutaneous tissue at wound entrance with high power (100×). High power confirmed the feature of the miniscule gunpowder particles.
Figure 4. Histological section of subcutaneous tissue at wound entrance with high power (100×). High power confirmed the feature of the miniscule gunpowder particles. References
1. Cvetković D, Živković V, Juković F, Nikolić S, Double suicidal gunshot wounds to the heart: Forensic Sci Med Pathol, 2018; 14(2); 248-50
2. Raniero D, Del Balzo G, Vermiglio E, A hard way to die: When multiple lethal gunshots mean suicide: Int J Legal Med, 2022; 136(1); 179-87
3. Marzuk PM, Tardiff K, Hirsch CS, The epidemiology of murder-suicide: JAMA, 1992; 267(23); 3179-83
4. National Institute on Minority Health and Health Disparities [Internet]: Health Disparities and Minority Health Data Portal: Mortality Table, US Department of Health and Human Services [cited 2025 Apr 8]. Available from: https://hdpulse.nimhd.nih.gov/data-portal/mortality/table
5. Karger B, On the significance of the number of shots in suspected self-inflicted gunshot injuries: Forensic Sci Int, 1995; 76(2–3); 93-100
6. DiMaio VJM: Gunshot wounds: Practical aspects of firearms, ballistics, and forensic techniques, 1999, Boca Raton, CRC Press
7. Schyma C, Madea B, Determination of vitality and direction of gunshot wounds: Forensic Sci Int, 2008; 179(2–3); 101-11
8. Karger B, Forensic ballistics: Forensic Pathology Reviews, 2008; 5; 139-72, Totowa, NJ, Humana Press
9. Drummer OH, Drug testing in oral fluid: Clin Biochem Rev, 2006; 27(3); 147-59
10. Kintz P, Postmortem toxicology: Analytical Techniques in Forensic Toxicology, 2016; 413-43, London, Elsevier
Figures
Figure 1. Anterior chest showing 3 entrance gunshot wounds clustered in the precordial region. Arrows denote wound sites. No soot or stippling visible externally. No visible soot or gunpowder stippling around wounds. Note the medical artifacts caused by a LUCAS device used for chest compressions.Figure 2. Three exit gunshot wounds on the left side of the back and left flank region (blue arrow) associated with 3 entrance wounds on the chest. The margins showed lacerated features.Figure 3. Histological section (H&E stain, 40× magnification) of subcutaneous tissue demonstrating sparse embedded gunpowder particles along the wound tract, consistent with close-range discharge. Disruption of the subcutaneous tissue, coagulation necrosis, and gunpowder particles deposit.Figure 4. Histological section of subcutaneous tissue at wound entrance with high power (100×). High power confirmed the feature of the miniscule gunpowder particles. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133