31 December 2025: Articles 
Percutaneous Arterial Closure for Inadvertent Subclavian Artery Cannulation During Central Venous Catheterization: A Case Report
Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents
Guangrong ZiDOI: 10.12659/AJCR.950797
Am J Case Rep 2025; 26:e950797






Abstract
BACKGROUND: Arterial injury during central venous catheterization (CVC) occurs in 0.1% to 2.7% of cases and can lead to serious complications, such as arterial occlusion, embolism, pseudoaneurysm, vessel rupture, and life-threatening hemorrhage. These risks are particularly concerning in critically ill patients, especially those receiving anticoagulation or with acute coagulopathy.
CASE REPORT: We report the case of an 81-year-old woman with a complex medical history, including chronic heart failure, atrial fibrillation, chronic obstructive pulmonary disease (COPD), and chronic kidney disease, whose left subclavian artery was accidentally punctured during central venous catheterization (CVC). The injury was managed successfully by removing the catheter and performing percutaneous arterial closure. The repair involved image-guided percutaneous vascular suturing, using fluoroscopy and real-time contrast imaging. Before the procedure, color Doppler ultrasonography was used to assess the injury’s size and location, while CT angiography evaluated the surrounding vasculature for complications, including arterial rupture or significant bleeding. The postoperative recovery was uneventful, with no signs of pseudoaneurysm or arteriovenous fistula. The patient maintained stable hemodynamics throughout the recovery period and exhibited no signs of further vascular complications.
CONCLUSIONS: Percutaneous suturing is a safe and effective method for managing mild arterial injuries during central venous catheterization (CVC), especially in patients with complex comorbidities. This approach provides precise hemostasis, minimizes vascular trauma, and offers a minimally invasive solution to prevent significant complications, ensuring a smooth recovery.
Keywords: Catheterization, Central Venous, Subclavian Artery, Vascular Closure Devices, Humans, Female, Aged, 80 and over, Vascular System Injuries
Introduction
Central venous catheterization is a routine procedure in clinical practice, commonly used in critical care and therapeutic interventions. Despite its routine nature, complications remain significant and warrant caution [1]. Arterial injury, particularly with large-bore catheters, is one of the most frequent complications of this procedure. Delayed recognition of arterial injury can lead to serious outcomes, including pseudoaneurysm, thrombosis, and arteriovenous fistula. Although ultrasound guidance reduces the risk of arterial puncture, arterial injuries may still occur despite its use [2]. Subclavian artery (SCA) injury poses unique challenges due to its deep location and non-compressibility, often resulting in ineffective manual hemostasis and increased risk of uncontrolled bleeding [3]. In this case, despite the patient’s hypotension and chronic hypoxia, identifying the bleeding source was initially difficult. The deep location of the SCA and the rapid onset of bleeding likely delayed recognition of the injury, as the blood was initially indistinguishable from venous or other hemorrhage sources. Recent advancements in endovascular repair techniques, such as percutaneous vascular suturing devices and covered stents, have emerged as safer and more effective treatment options for complications from arterial punctures [4]. This report details an accidental left subclavian artery puncture during central venous catheterization, which was successfully managed through catheter removal followed by percutaneous arterial suturing, preventing further complications. This case highlights the potential of endovascular therapy in managing arterial punctures, particularly when conventional methods fail to achieve adequate hemostasis, providing a minimally invasive and safe alternative. By examining the broader application of percutaneous vascular suturing devices in similar cases, this case aims to provide practical guidance for managing such events and promote the clinical adoption of endovascular techniques.
Case Report
The patient was an 81-year-old woman with a 20-year history of recurrent palpitations. Recently, her palpitations had worsened, accompanied by dizziness and nausea. She had multiple comorbidities, including chronic heart failure, paroxysmal atrial fibrillation, hypertension, type 2 diabetes mellitus, chronic obstructive pulmonary disease (COPD), and chronic kidney disease (CKD). Over 20 years ago, she underwent radiofrequency ablation for atrial fibrillation and has been on long-term Edoxaban Tosylate therapy. A second ablation was performed five years ago for recurrent atrial fibrillation, which led to symptomatic improvement. Physical examination revealed hypotension (68/57 mmHg), tachycardia (120 bpm), and mild bilateral lower limb edema. Laboratory tests showed anemia (hemoglobin 99 g/L), elevated serum creatinine (230 μmol/L), and proteinuria (1+). Electrocardiography revealed 2: 1 atrial flutter, and echocardiography demonstrated left ventricular hypertrophy, biatrial enlargement, pulmonary hypertension (PASP ~86 mmHg), and moderate tricuspid regurgitation. Due to hypotension and inadequate peripheral venous access, a left subclavian vein catheterization was performed to improve fluid administration. The skin was disinfected, a sterile drape was applied, and local anesthesia was administered. The puncture needle was inserted at a 30°angle toward the sternal notch. Dark red blood was aspirated and mistakenly identified as venous. A guidewire and deep venous catheter were subsequently inserted. After the procedure, a mild pulsatile blood flow was observed slowly refluxing within the catheter. Arterial blood gas analysis showed a PaO2 of 68 mmHg, raising suspicion of catheter misplacement into the left subclavian artery. Emergent cervical vascular ultrasonography and contrast-enhanced CT confirmed that the catheter was in the left subclavian artery, with its tip at the arterial origin. No arteriovenous fistula was observed (Figure 1A–1C). Given the deep anatomical location of the left subclavian artery and its non-compressibility, along with the patient’s overall condition, percutaneous arterial suturing was selected for vascular repair. A new left subclavian vein catheterization was conducted before the procedure. Left subclavian vein angiography was performed, with no contrast agent leakage observed (Figure 2A, 2B). After routine disinfection, sterile draping, and local anesthesia, successful puncture of the left radial artery was achieved. A 7F radial artery sheath was placed, and under fluoroscopic guidance, a JR4.0 guiding catheter was advanced to the proximal segment of the left subclavian artery. Angiography revealed the central venous catheter traversing the left subclavian artery without significant contrast extravasation. A guidewire was advanced through the injured arterial segment into the ascending aorta. A 5.0×8 mm NC TREK balloon was placed proximal to the injury site over the guidewire and continuously inflated to occlude blood flow. A 6F ExoSeal (Cordis) vascular closure device was deployed through the misplaced catheter, sealing the puncture site. Gradual withdrawal of the device was performed while monitoring bleeding from the indicator tube. When bleeding ceased, indicating that the device tip had reached the correct extravascular position adjacent to the arterial wall, the occlusion mechanism was deployed. The device was then removed, and gentle manual pressure was applied to the puncture site. Follow-up angiography demonstrated intact flow in the left subclavian artery, with no contrast extravasation (Figure 3A–3C). The procedure was completed, and the patient was transferred to the cardiac intensive care unit (CICU). Postoperatively, the patient recovered well without complications such as pseudoaneurysm, arterial dissection, or vascular occlusion.
Discussion
Despite significant progress in imaging-guided techniques, arterial injury remains a well-recognized complication of central venous catheterization. Although relatively uncommon, such events can result in severe and potentially life-threatening consequences. Subclavian artery (SCA) injuries are particularly challenging owing to the vessel’s deep anatomical course and lack of compressibility, which limit the effectiveness of conventional hemostatic maneuvers. These anatomical and technical factors underscore the need for prompt recognition and effective management to minimize morbidity and mortality [5].
This case highlights the complexity of managing an SCA injury in a high-risk patient with multiple comorbidities, including chronic heart failure, atrial fibrillation, and chronic kidney disease. The combination of deep vascular anatomy and hemodynamic instability increased the likelihood of inadvertent arterial puncture and delayed recognition. Nevertheless, rapid diagnosis and timely intervention facilitated successful management, preventing secondary complications such as hematoma formation or pseudoaneurysm development [6].
Traditional management of arterial injuries from CVC includes manual compression, endovascular interventions, and open surgical repair. While percutaneous stent graft implantation is commonly used in such cases, newer approaches, such as percutaneous arterial suturing, provide an effective and minimally invasive alternative, particularly for minor arterial injuries in anatomically challenging regions, like the SCA [7]. Endovascular repair has become increasingly favored due to its minimally invasive nature; however, percutaneous suturing allows for precise closure of the arterial defect with minimal tissue trauma and a faster recovery [8].
In the present case, percutaneous suturing was selected, given the limited extent of arterial injury and the patient’s frail condition. The method provided accurate closure with minimal vascular manipulation, offering an optimal balance between efficacy and safety [9]. Imaging played an indispensable role throughout diagnosis and treatment. Preoperative color Doppler ultrasonography and CT angiography accurately localized the puncture site and delineated the extent of vascular injury, while intraoperative digital subtraction angiography and fluoroscopic guidance provided real-time visualization that enhanced procedural precision and ensured complete hemostasis [10].
This case highlights the importance of accurate diagnosis and timely intervention in managing inadvertent arterial punctures during CVC. The use of percutaneous arterial suturing, combined with advanced imaging techniques, offers a safe and effective approach, particularly in high-risk patients with complex comorbidities. As technology and devices continue to evolve, these minimally invasive methods are expected to improve, allowing for even greater precision in managing such complications.
Conclusions
This case illustrates the successful management of an inadvertent perforation of the left subclavian artery during central venous catheterization. Percutaneous arterial repair using a vascular closure device avoided the need for open surgery and minimized postoperative complications. Minimally invasive techniques, especially in cases of deep arterial injuries where manual compression is ineffective, have shown favorable outcomes. Key clinical lessons include the importance of timely recognition and the role of percutaneous techniques in managing complex arterial injuries.
Figures
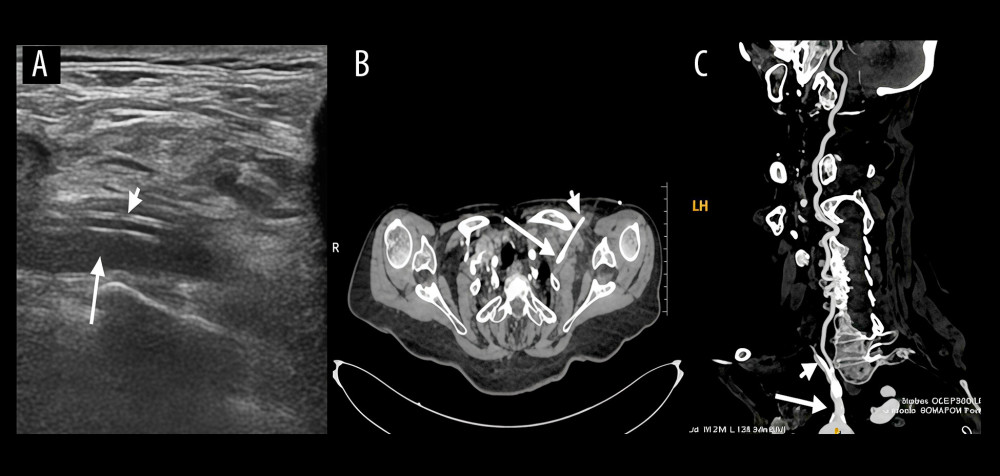 Figure 1. (A, B) Duplex ultrasonography of the cervical vessels and contrast-enhanced CT confirm the malposition of the central venous catheter (short arrow) within the left subclavian artery (long arrow). (C) Maximum intensity projection (MIP) reconstruction demonstrates the central venous catheter located in the left subclavian artery (long arrow), with the catheter tip (short arrow) positioned near the arterial origin.
Figure 1. (A, B) Duplex ultrasonography of the cervical vessels and contrast-enhanced CT confirm the malposition of the central venous catheter (short arrow) within the left subclavian artery (long arrow). (C) Maximum intensity projection (MIP) reconstruction demonstrates the central venous catheter located in the left subclavian artery (long arrow), with the catheter tip (short arrow) positioned near the arterial origin. 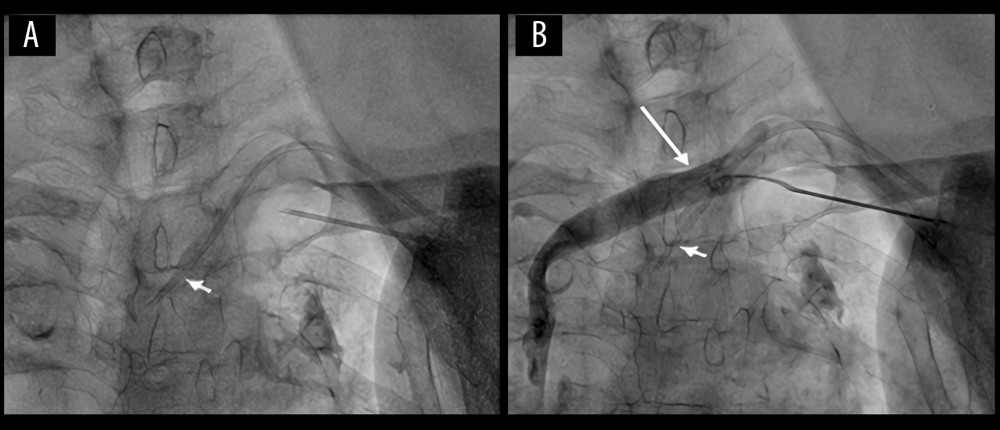 Figure 2. (A, B) Real-time fluoroscopy shows the malpositioned central venous catheter (short arrow). Contrast venography of the left subclavian vein (long arrow) demonstrates no evidence of contrast extravasation.
Figure 2. (A, B) Real-time fluoroscopy shows the malpositioned central venous catheter (short arrow). Contrast venography of the left subclavian vein (long arrow) demonstrates no evidence of contrast extravasation. 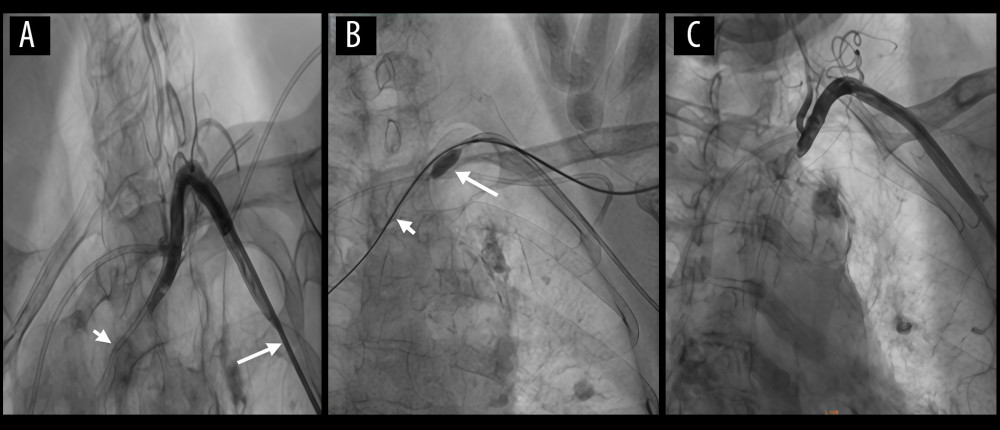 Figure 3. (A) Angiography performed with a JR4.0 catheter (long arrow) demonstrates the central venous catheter (short arrow) malpositioned within the left subclavian artery. (B) A 5.0×8 mm NC TREK balloon (long arrow) was continuously inflated to achieve temporary flow occlusion. A 6F ExoSeal vascular closure device (Cordis) (short arrow) was then deployed through the malpositioned central venous catheter and gradually withdrawn to close the injured vessel. (C) Postoperative follow-up angiography shows no evidence of arterial aneurysm or dissection.
Figure 3. (A) Angiography performed with a JR4.0 catheter (long arrow) demonstrates the central venous catheter (short arrow) malpositioned within the left subclavian artery. (B) A 5.0×8 mm NC TREK balloon (long arrow) was continuously inflated to achieve temporary flow occlusion. A 6F ExoSeal vascular closure device (Cordis) (short arrow) was then deployed through the malpositioned central venous catheter and gradually withdrawn to close the injured vessel. (C) Postoperative follow-up angiography shows no evidence of arterial aneurysm or dissection. References
1. Kusminsky RE, Complications of central venous catheterization: J Am Coll Surg, 2007; 204(4); 681-96
2. McGee DC, Gould MK, Preventing complications of central venous catheterization: N Engl J Med, 2003; 348(12); 1123-33
3. Guilbert MC, Elkouri S, Bracco D, Arterial trauma during central venous catheter insertion: Case series, review and proposed algorithm: J Vasc Surg, 2008; 48(5); 918-25
4. Thalhammer C, Kirchherr AS, Uhlich F, Postcatheterization pseudoaneurysms and arteriovenous fistulas: Repair with percutaneous implantation of endovascular covered stents: Radiology, 2000; 214(1); 127-31
5. Dixon OGB, Smith GE, Carradice D, Chetter IC, A systematic review of management of inadvertent arterial injury during central venous catheterisation: J Vasc Access, 2017; 18(6); 495-502
6. Branco BC, Boutrous ML, DuBose JJ, Outcomes after subclavian and axillary artery injuries: A National Trauma Data Bank analysis: J Vasc Surg, 2016; 63(3); 702-9
7. Pikwer A, Acosta S, Kölbel T, Management of inadvertent arterial catheterisation associated with central venous access procedures: Eur J Vasc Endovasc Surg, 2009; 38; 707-14
8. Trabattoni D, Bartorelli AL, Agrifoglio M, Montorsi P, Endovascular repair of iatrogenic subclavian artery perforations using the Hemobahn stent-graft: J Endovasc Ther, 2001; 8; 417-21
9. AlSheikh S, Aldossary MY, Najeeb R, Management of arterial trauma during central venous catheter insertion using a percutaneous suture-mediated closure device (Perclose ProGlide): A report of two cases and literature review: Signa Vitae, 2023; 19; 211-16
10. Fritz J, Efron DT, Fishman EK, Multidetector CT and three-dimensional CT angiography of upper extremity arterial injury: Emerg Radiol, 2015; 22; 45-52
Figures
Figure 1. (A, B) Duplex ultrasonography of the cervical vessels and contrast-enhanced CT confirm the malposition of the central venous catheter (short arrow) within the left subclavian artery (long arrow). (C) Maximum intensity projection (MIP) reconstruction demonstrates the central venous catheter located in the left subclavian artery (long arrow), with the catheter tip (short arrow) positioned near the arterial origin.Figure 2. (A, B) Real-time fluoroscopy shows the malpositioned central venous catheter (short arrow). Contrast venography of the left subclavian vein (long arrow) demonstrates no evidence of contrast extravasation.Figure 3. (A) Angiography performed with a JR4.0 catheter (long arrow) demonstrates the central venous catheter (short arrow) malpositioned within the left subclavian artery. (B) A 5.0×8 mm NC TREK balloon (long arrow) was continuously inflated to achieve temporary flow occlusion. A 6F ExoSeal vascular closure device (Cordis) (short arrow) was then deployed through the malpositioned central venous catheter and gradually withdrawn to close the injured vessel. (C) Postoperative follow-up angiography shows no evidence of arterial aneurysm or dissection. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133