22 December 2025: Articles 
Afebrile Recurrent Cellulitis Complicated by Linezolid-Induced Lactic Acidosis in an Elderly Patient
Unusual or unexpected effect of treatment, Adverse events of drug therapy, Educational Purpose (only if useful for a systematic review or synthesis)
Yanizbeth Yambó-Chévere BCDEF 1*, Rafael Bermúdez-Rivera BE 1,2DOI: 10.12659/AJCR.951194
Am J Case Rep 2025; 26:e951194






Abstract
BACKGROUND: Cellulitis typically presents with erythema, swelling, warmth, and systemic signs such as fever and leukocytosis. In older adults, immunosenescence and multimorbidity can blunt classical inflammatory responses, delaying diagnosis and complicating care. Linezolid, while effective against resistant gram-positive organisms, carries a risk of mitochondrial dysfunction and lactic acidosis during prolonged therapy.
CASE REPORT: We describe the case of an 87-year-old Puerto Rican woman with multiple comorbidities who experienced 4 hospitalizations in 6 months for recurrent cellulitis. Despite having visible inflammation, she consistently remained afebrile and without leukocytosis. Laboratory findings demonstrated a persistently elevated C-reactive protein level and erythrocyte sedimentation rate. Wound cultures revealed polymicrobial organisms, including Pseudomonas aeruginosa, Klebsiella pneumoniae, and Stenotrophomonas maltophilia. Broad-spectrum antibiotics were used, including linezolid at 600 mg twice daily, with an estimated total exposure of approximately 8 weeks across hospitalizations and outpatient treatment. Renal and hepatic function were monitored and remained stable throughout. Ultrasound imaging did not reveal abscess or osteomyelitis. During the final hospitalization, she developed lactic acidosis (lactate 2.5-3.1 mmol/L), in the absence of shock or hypoxemia, suggesting linezolid-induced mitochondrial toxicity. The patient died 2 days after discharge.
CONCLUSIONS: This case underscores the diagnostic challenges of afebrile cellulitis in frail older adults and the importance of careful antimicrobial stewardship. Clinicians should maintain vigilance for linezolid-induced lactic acidosis during extended therapy, particularly in patients with atypical presentations. The integration of biomarker trends into decision-making, prioritization of preventive strategies, and coordination of geriatric care are essential to improve outcomes in this vulnerable population.
Keywords: Age Factors, Cellulitis, immunosenescence, Lactic Acid, linezolid, Humans, Female, Acidosis, Lactic, Aged, 80 and over, Anti-Bacterial Agents, Recurrence
Introduction
Cellulitis is an acute bacterial infection of the dermis and subcutaneous tissues characterized by localized erythema, swelling, warmth, and tenderness [1,2]. Globally, cellulitis contributes substantially to morbidity and hospitalization, particularly among older adults, who are at increased risk due to comorbidities, frailty, and impaired skin integrity [3,4]. Linezolid is increasingly used in complex infections but can cause mitochondrial toxicity and lactic acidosis with prolonged exposure. The rarity of afebrile recurrent cellulitis complicated by linezolid-associated lactic acidosis specifically in elderly, immunosuppressed patients make this case especially instructive. To the best of our knowledge, no prior reports describe this specific combination of afebrile recurrent cellulitis, prolonged linezolid exposure, and lactic acidosis in a frail, elderly patient with multiple hospitalizations. In contrast to reports that highlight the typical presentation of fever and leukocytosis as hallmark features, our patient demonstrated a profoundly blunted inflammatory response across multiple hospitalizations.
Diagnosis in elderly populations can be especially challenging. Classic signs of infection such as fever and leukocytosis may be absent due to immunosenescence, a progressive decline in immune system function associated with aging [5–7]. This atypical presentation often leads to delayed recognition, inappropriate treatment, and increased risk of recurrence or progression to severe infection. Importantly, this case adds value by illustrating how age-related immune dysregulation (immunosenescence) and repeated infectious episodes can not only delay diagnosis but can also potentiate susceptibility to adverse drug reactions, such as mitochondrial toxicity and lactic acidosis. This mechanistic connection reinforces the need to reframe clinical expectations in elderly patients and underscores the complex interplay between host factors and treatment effects. Our case illustrates how misattributing elevated lactate levels to infection alone, without considering cumulative linezolid exposure, can delay recognition of a potentially fatal drug toxicity.
Recurrent cellulitis, defined as 2 or more episodes within a specified timeframe, is associated with underlying conditions such as venous insufficiency, lymphedema, and chronic ulcers. These risk factors significantly increase the likelihood of recurrence and hospitalization [8]. Preventive and therapeutic strategies require thorough evaluation of comorbidities and tailored interventions to reduce recurrence risk.
Treatment regimens often involve broad-spectrum antibiotics, particularly in patients with resistant organisms or polymicrobial infections. Linezolid, an oxazolidinone antibiotic with strong efficacy against multidrug-resistant gram-positive bacteria, is widely used in complicated skin and soft tissue infections. However, prolonged therapy is associated with adverse effects, including mitochondrial toxicity and lactic acidosis [9,10]. These complications introduce diagnostic uncertainty in frail elderly patients, in whom systemic inflammatory markers can be elevated due to infection, drug toxicity, or both.
Case Report
We describe an 87-year-old Puerto Rican woman with a medical history of hypertension, hyperlipidemia, hypothyroidism, type 2 diabetes mellitus, systemic lupus erythematosus, psoriasis, and pacemaker placement for mitral valve hypertrophy. She was hospitalized 4 times over 6 months for recurrent cellulitis. Her home medications included prednisone (5 mg daily) for systemic lupus erythematosus, levothyroxine for hypothyroidism, and standard therapies for hypertension, diabetes, and hyperlipidemia.
At the first admission, she presented with a chronic ulcer on the right lower leg, with erythema, edema, and purulent discharge extending to bilateral upper extremities. Laboratory test results showed an elevated C-reactive protein (CRP) level of 9.8 mg/dL and an erythrocyte sedimentation rate (ESR) of 110 mm/h, but she remained afebrile, with normal white blood cell counts. Wound cultures isolated
The second admission occurred 1 month later, with recurrent cellulitis involving the right leg and upper limbs. The CRP level was 1.89 mg/dL, and ESR was 119 mm/h, again without fever or leukocytosis.
She received linezolid 600 mg twice daily for 10 days as an inpatient, for culture-confirmed
The third admission involved worsening infection with new ulcerations on the legs and arms. The CRP level was 1.10 mg/dL, and ESR, 102 mm/h. Wound cultures identified
In total, her cumulative linezolid exposure was approximately 42 to 56 days over a 6-month period, combining inpatient and outpatient use. Throughout these hospitalizations, she continued her home medications, including low-dose prednisone (5 mg daily) for systemic lupus erythematosus. No other mitochondrial-toxic medications (eg, antiretrovirals, chloramphenicol) were administered. Renal and hepatic function remained stable across all admissions. Imaging studies were performed during each admission, to evaluate for deep infection. Bedside and inpatient ultrasounds consistently showed no evidence of abscess or osteomyelitis. Magnetic resonance imaging was not pursued given the stable imaging findings and absence of systemic toxicity until the final admission.
During the fourth admission, she presented with persistent bilateral cellulitis and bacteremia. Significant elevation in inflammatory markers (CRP 11.1 mg/dL, ESR >110 mm/h) was noted again. The serum lactate level was elevated, ranging from 2.5 to 3.1 mmol/L, in the absence of hypoperfusion, shock, or hypoxemia. Given her prolonged linezolid exposure and lack of sepsis, mitochondrial toxicity was suspected. Linezolid was discontinued, and broad supportive care was provided. She died peacefully 2 days after discharge.
Discussion
Recurrent cellulitis in older adults is a complex condition shaped by multiple clinical and systemic factors. This case emphasizes the interplay of atypical presentation, antimicrobial toxicity, and fragmented healthcare delivery in determining outcomes. In elderly, immunosuppressed patients, the absence of fever or leukocytosis can obscure the diagnosis of infection. In such contexts, clinicians should not rely solely on classic clinical signs but should incorporate biomarkers and culture results into diagnostic and therapeutic decision-making [5,11].
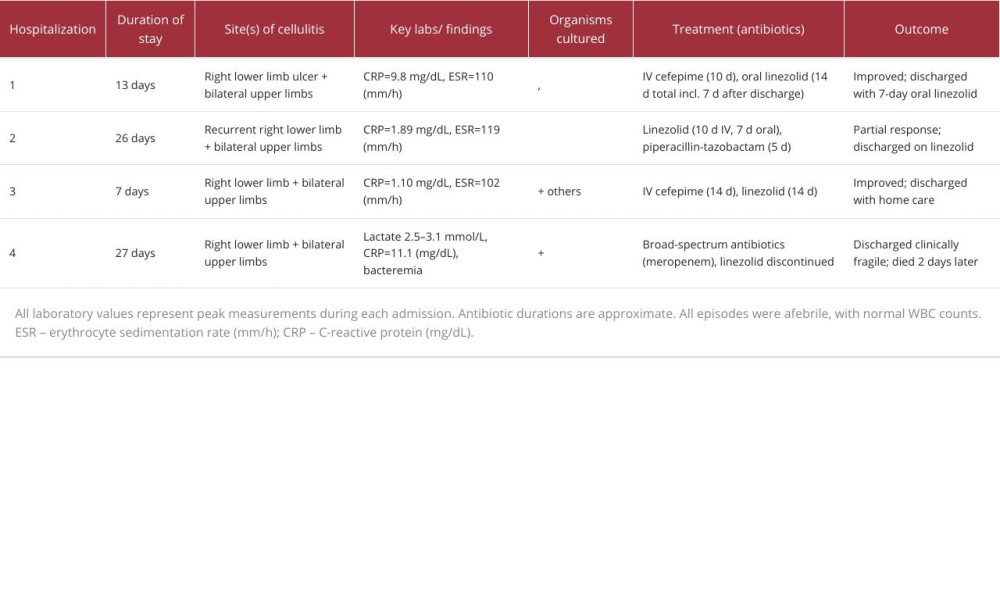
As summarized in Table 1 and Figure 1, the patient’s hospitalizations were marked by persistent inflammation, changing microbial flora, and prolonged cumulative linezolid exposure (approximately 42–56 days). During the final hospitalization, she developed lactic acidosis, with lactate levels ranging from 2.5 to 3.1 mmol/L, in the absence of hypotension, hypoxemia, or overt signs of sepsis. This clinical picture is consistent with prior case reports of linezolid-associated mitochondrial toxicity, particularly in elderly patients or patients with comorbidities receiving extended courses [9,10,12–14].
However, alternative contributors to lactic acidosis cannot be fully excluded. Diabetes-related metabolic derangements, subclinical hypoperfusion, and occult infection not evident in vital signs or imaging may have played a role in our patient’s case. These were considered less likely given the patient’s stable renal and hepatic function, absence of systemic shock, and the close temporal relationship to cumulative linezolid exposure. Nonetheless, this highlights the diagnostic uncertainty intrinsic to single-patient observations. In keeping with case-report standards, we interpret the association between linezolid and lactic acidosis as probable rather than definitive. The inference is supported by the timing of symptom onset, exclusion of more common alternative causes, and clinical improvement efforts focused on discontinuing the suspected agent.
Our findings are consistent with those of previous reports of linezolid-induced lactic acidosis, which typically occurs after more than 2 weeks of therapy in frail or elderly patients [13,14]. For example, Santos-Vazquez et al described a case involving a younger adult with a soft tissue infection and classic systemic signs of sepsis [13]. In contrast, our case is distinguished by its combination of recurrent afebrile cellulitis, blunted systemic inflammatory response, and the development of lactic acidosis in the absence of shock or hypoxemia. These findings underscore the unique diagnostic and therapeutic challenges posed by immunosenescence and cumulative drug exposure in the frail elderly. Decisions to continue linezolid despite evolving culture profiles should be individualized, balancing antimicrobial susceptibility, oral step-down options, tissue penetration, and patient frailty within an antimicrobial stewardship framework.
Although gram-positive organisms were not isolated in the last 3 hospitalizations, linezolid was continued based on prior efficacy and as a precaution against potential gram-positive co-infection, particularly in the context of immunosuppression and polymicrobial skin infections. This approach reflects a common clinical practice in complex cases in which cultures can miss transient or deep-seated organisms. However, this strategy must be weighed against the known risks of prolonged linezolid exposure. The lack of gram-positive isolates could have prompted reassessment of the regimen, especially once gram-negative coverage was established. This case exemplifies the clinical tension between empiric coverage and culture-directed therapy, reinforcing the need for ongoing re-evaluation of antimicrobial regimens as new microbiologic data emerge.
Care coordination also influences outcomes. Limited interoperability of electronic health records and restricted access to long-term care services can disrupt continuity in resource-limited settings. Streamlined discharge planning and early outpatient follow-up are essential to prevent recurrence and mitigate adverse outcomes [3,15,16].
Ultimately, optimal management of recurrent cellulitis in frail older adults requires more than antibiotics. Clinicians must integrate microbiologic data with vigilant toxicity monitoring, implement preventive strategies, such as edema control and skin care, and advocate for systemic improvements that enhance care continuity and patient safety.
Conclusions
This case underscores the diagnostic challenges of afebrile cellulitis in frail older adults and highlights the importance of culture-guided antimicrobial stewardship. The patient’s prolonged cumulative exposure to linezolid, in the absence of sepsis, hypoxia, or organ failure, suggests a probable association between the antibiotic and the development of lactic acidosis. However, other potential contributors, including comorbid diabetes, underlying frailty, and possible subclinical hypoperfusion, cannot be fully excluded.
This case reinforces the need for rational antibiotic use, particularly in elderly or immunosuppressed populations, in which atypical presentations can lead to prolonged empiric therapy. Indiscriminate or precautionary continuation of broad-spectrum agents, like linezolid, especially without microbiologic confirmation, can result in avoidable harm. Clinicians must regularly re-evaluate antimicrobial regimens considering evolving culture data, patient risk factors, and treatment duration.
We advocate for vigilant toxicity monitoring, personalized care planning, and preventive strategies, such as edema control and coordinated follow-up, to optimize outcomes. Beyond emphasizing individual patient care, this case underscores the broader imperative to curb antibiotic overuse and preserve antimicrobial efficacy through targeted, evidence-based prescribing.
![Timeline of the patient’s 4 hospitalizations over 6 months. Each horizontal line represents the duration of a hospitalization. Green “×” markers indicate admission dates; red “×” markers indicate discharges. Annotations summarize site of infection, organisms isolated, peak inflammatory markers (C-reactive protein [CRP] and erythrocyte sedimentation rate [ESR]), and treatment regimens. Cumulative linezolid exposure across the first 3 hospitalizations totaled approximately 42 to 56 days and preceded the development of lactic acidosis during the fourth admission. All episodes were afebrile, with normal white blood cell counts.](https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e951194-g001.jpg&idArt=951194&w=1000)
References
1. Raff AB, Kroshinsky D, Cellulitis: A review: JAMA, 2016; 316(3); 325-37
2. Stevens DL, Bisno AL, Chambers HF, Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America: Clin Infect Dis, 2014; 59(2); e10-e52
3. Alvarado J, López-Cepero A, Pérez CM, Epidemiological transition and chronic disease trends in Puerto Rico: 2000–2020: P R Health Sci J, 2021; 40(1); 10-18
4. Hay RJ, Johns NE, Williams HC, The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions: Lancet, 2014; 384(9942); 76-83
5. Aiello AE, Malinis M, Infections in the elderly: Lancet Infect Dis, 2022; 22(9); e303-e13
6. Gavazzi G, Krause KH, Ageing and infection: Lancet Infect Dis, 2002; 2(11); 659-66
7. Nikolich-Žugich J, The twilight of immunity: Emerging concepts in aging of the immune system: Nat Immunol, 2018; 19(1); 10-19
8. Cannon J, Rajakaruna G, Wickremaratne D, Risk factors for recurrent cellulitis: A systematic review and meta-analysis: J Infect, 2018; 77(6); 417-23
9. De Vriese AS, Coster RV, Smet J, Linezolid-induced inhibition of mitochondrial protein synthesis: Clin Infect Dis, 2006; 42(8); 1111-17
10. Herrera S, Daza M, Ramírez P, Mitochondrial toxicity and lactic acidosis related to linezolid: Systematic review and meta-analysis: Clin Infect Dis, 2022; 74(3); 444-52
11. High KP, Bradley SF, Gravenstein S, Clinical practice guideline for the evaluation of fever and infection in older adult residents of long-term care facilities: 2008 update by the Infectious Diseases Society of America: Clin Infect Dis, 2009; 48(2); 149-71
12. Nagai J, Takano M, Iwai Y, Risk factors for lactic acidosis during linezolid therapy: A case-control study: Clin Drug Investig, 2020; 40(7); 619-27
13. Santos-Vazquez G, Aldana-Vazquez JY, Linezolid-induced pancreatitis, hypoglycemia, and lactic acidosis: Case report and literature review: ACP Clin Cases, 2025; 4(3); aimcc.2024.0924
14. Chaudhri M, Costanzo E, Fareen N, Patel M, Linezolid-induced lactic acidosis: A case report: Cureus, 2024; 16(12); e76618
15. Manca DP, Do electronic medical records improve quality of care?: CMAJ, 2015; 187(5); E128-E29
16. Torres I, Mattei J, Rodríguez-Díaz CE, Puerto Rico’s health system resilience post-Hurricane Maria: Implications for disaster preparedness in a time of climate change: Lancet Planet Health, 2017; 1(5); e209-e10
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133