22 December 2025: Articles 
Asymptomatic Lung Adenocarcinoma With Cardiac Metastasis at Initial Diagnosis: A Case Report
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare disease
Tianyu Jin ABDEF 1, Yongzhong Jiang ABD 1, Yong Song DEG 2*DOI: 10.12659/AJCR.951223
Am J Case Rep 2025; 26:e951223






Abstract
BACKGROUND: Cardiac metastasis from lung cancer is rare and usually involves the pericardium. Myocardial or endocardial metastases are even less common and are often diagnosed postmortem or during late-stage disease when severe symptoms appear. Early detection in asymptomatic patients is challenging due to the heart’s unique anatomy and the risks associated with myocardial biopsy. However, advances in imaging, particularly positron emission tomography-computed tomography (PET-CT) combined with magnetic resonance imaging (MRI), enable non-invasive diagnosis. Identifying such lesions before clinical symptoms emerge may help prolong survival.
CASE REPORT: A man in his 50s was diagnosed with right lower-lobe lung adenocarcinoma by needle biopsy and admitted for surgical evaluation. During preoperative staging, PET-CT and MRI revealed a lesion in the left ventricular myocardium, although the patient had no cardiac symptoms. Imaging suggested a metastatic focus. Due to the high risk of biopsy, pathological confirmation was deferred. The patient received systemic treatment combining chemotherapy and targeted therapy. After 2 treatment cycles, follow-up cardiac MRI showed that the lesion had decreased in size from 23×13×29 mm to 17×12×26 mm.
CONCLUSIONS: Myocardial metastasis from lung adenocarcinoma is extremely rare, especially in asymptomatic individuals. In such cases, PET-CT is essential for distant metastasis screening, and MRI is the most appropriate tool to evaluate cardiac lesions when biopsy is unsafe. Early detection enables timely systemic therapy and can prevent life-threatening events. Clinical efforts should focus on improved screening of high-risk patients and development of individualized treatment strategies.
Keywords: Heart Neoplasms, lung neoplasms, Magnetic Resonance Imaging, Humans, Male, Middle Aged, Adenocarcinoma of Lung, Positron Emission Tomography Computed Tomography, Adenocarcinoma, Asymptomatic Diseases
Introduction
Cardiac metastatic tumors are extremely rare in clinical practice and are mostly detected during autopsies of cancer patients, accounting for approximately 1.5% to 20% [1]. It has been reported that the incidence of cardiac metastatic tumors is about 1.8% [2], which is much higher than that of primary cardiac tumors (0.009%) [3]. Melanoma is a common primary source [4], whereas reports of cardiac metastasis originating from lung cancer remain relatively scarce.
Cardiac metastasis is typically characterized by occult presentation, often identified upon the manifestation of overt clinical symptoms, such as pericardial effusion or acute myocardial infarction. However, when complicated by cardiovascular events, patients are already in the terminal stage of cancer. At this point, treatment efficacy is poor, and the survival time is significantly shortened. With the advancement of modern imaging techniques, early detection of metastatic lesions via non-invasive examination has become feasible. In this case, cardiac metastasis was diagnosed via PET-CT and cardiac MRI before the patient developed clinical symptoms. Timely intervention resulted in effective control of the metastatic lesion. This may prolong patient survival.
Case Report
A male patient in his 50s was diagnosed with adenocarcinoma of the right lower-lung lobe via percutaneous lung biopsy. He had a smoking history of 20 packs per year (0.5 pack/day for 40 years). Chest CT revealed a 4×3 cm pure solid mass in the lung, with pleural traction. Enlarged mediastinal lymph nodes were also observed.
To rule out distant metastases, a PET-CT scan was performed. Besides indicating metastases in the 3A, 4R, 9R, and 10R mediastinal lymph node regions, the PET-CT showed a massive area of abnormal FDG hypermetabolism in the left ventricular myocardial region, with a SUVmax of 12.69 (Figure 1). No abnormalities were detected during cardiac auscultation. The electrocardiogram showed peaked T waves in leads V2 and V3, while echocardiography revealed no myocardial abnormalities.
For further diagnosis, an enhanced cardiac MRI was immediately performed. The MRI results revealed specific findings in the left ventricle, with strip-like areas identified in the basal inferolateral and anterolateral regions. These areas showed slightly hyperintense signals on T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI). On diffusion-weighted imaging (DWI), they presented relatively high signals. On apparent diffusion coefficient (ADC), they demonstrated slightly low signals. The size of these areas was approximately 23×13×29 mm (Figure 2). No obvious pericardial effusion was noted. Given the anatomical and functional uniqueness of the heart, which made biopsy sampling extremely challenging, myocardial biopsy was deferred after multidisciplinary discussion. A preliminary diagnosis of the cardiac lesion as a metastatic focus from lung cancer was made, and the patient was recommended to receive anti-tumor treatment first.
Genetic testing of the lung cancer revealed an EGFR exon 21 mutation (L861Q) with an abundance of 51.88%, TP53 mutation with 13.73%, MET missense mutation with 43.6%, PIK3CA missense mutation with 12.03%, PD-L1 TPS of 65%, and CPS of 65. According to the NCCN Clinical Practice Guidelines in Oncology and the Chinese Society of Clinical Oncology (CSCO) Guidelines for the Diagnosis and Treatment of Non-Small Cell Lung Cancer (NSCLC), both the second-generation EGFR tyrosine kinase inhibitor (TKI) afatinib and the third-generation EGFR-TKI Osimertinib are categorized as Category I preferred options for the first-line treatment of patients with advanced NSCLC harboring the EGFR exon 21 L861Q mutation. However, for the specific EGFR L861Q mutation subtype, multiple retrospective studies and real-world analyses have shown that afatinib is associated with longer median progression-free survival (mPFS) and median overall survival (mOS) than Osimertinib. Based on these results, the treatment regimen of AP chemotherapy (pemetrexed + cisplatin) combined with afatinib was selected.
Cardiac MRI demonstrated a reduction in the size of the myocardial metastatic lesion, from 23×13×29 mm to 17×12×26 mm, following 2 courses of treatment (6 weeks). During the treatment period, we regularly rechecked myocardial markers and NT-proBNP, and all indicators were within normal ranges. Electrocardiograms (ECGs) were also re-examined upon each hospital admission, with no other specific changes observed. Currently, the patient has experienced no cardiovascular events.
Discussion
In patients with advanced lung cancer, distant metastases most commonly occur in organs such as bones, brain, and liver, while cardiac metastases are extremely rare. Cancer cells can involve the heart through direct spread, lymphatic metastasis, and venous (inferior vena cava) metastasis [5]. The most common site of cardiac metastasis is the pericardium (accounting for 88%), followed by the myocardium (5–11%), and metastases to the endocardium are very rare (<3%) [6]. The mechanism of cardiac metastasis remains unclear. Circulating tumor cells (CTCs) may be the “seeds” of tumor metastasis. They detach from the primary lesion, enter the bloodstream, and then colonize the myocardium or pericardium. Its colonization ability may be associated with the tumor microenvironment [7].
The clinical manifestations caused by cardiac metastasis are important factors for successful diagnosis, which are closely related to the size, location, and degree of invasion of the metastatic lesions [8]. We reviewed multiple studies, all of which emphasized that the diagnosis of cardiac metastasis was only confirmed after the detection of clinical symptoms of varying severity [9–11]. Symptoms related to arrhythmia, such as chest tightness, chest pain, and palpitations, are the most common but lack specificity [8]. Additionally, anti-tumor treatments including pharmacotherapy and local radiotherapy may themselves induce various cardiovascular events [12,13], which renders the diagnosis of cardiac metastasis extremely challenging. One study reported a case of a lung cancer patient who presented with chest pain; the initial diagnosis was suspected to be acute myocardial infarction. However, emergency coronary angiography revealed no coronary artery stenosis. Subsequent echocardiography detected an intracardiac mass in the ventricular myocardium. The patient died 1 month later, and autopsy finally confirmed that the mass was a cardiac metastatic lesion from lung cancer [10]. Additionally, when patients present with symptoms related to dyspnea or heart failure, it may indicate pericardial effusion caused by pericardial metastasis, and the diagnosis of pericardial metastasis can be confirmed via pericardiocentesis and fluid analysis [14]. Another study also reported a case where lung cancer metastases invaded the left ventricular myocardium, leading to symptoms of cardiac tamponade [9]. The clinical manifestations mentioned in the above studies mostly occur in the terminal stage of cancer. Even if the diagnosis of cardiac metastasis is confirmed at this point, therapeutic intervention is rarely effective in prolonging patient survival [15]. In contrast, the patient in the present case was diagnosed with cardiac metastasis before the onset of symptoms. This allowed us to obtain an earlier intervention window, successfully preventing the occurrence of malignant cardiovascular events (such as arrhythmia and cardiac tamponade), which highlights the special value of this case in clinical practice.
The diagnosis of cardiac metastasis is extremely challenging. Imaging examinations are characterized by non-invasiveness, safety, and convenience. Echocardiography and electrocardiography are the first-line options, yet they are insufficient to confirm the diagnosis and distinguish between benign and malignant lesions [16,17]. For patients with solid lung cancer similar to this case, timely completion of PET-CT examination is recommended. Precisely because PET-CT scans the entire body, we were able to detect myocardial abnormalities in a timely manner. However, inflammatory cells associated with myocardial ischemia, infarction [18], or other physiological changes can also increase FDG uptake, leading to potential false positives in PET-CT results. Cardiac MRI is the optimal imaging modality for evaluating cardiac metastatic disease, particularly exhibiting high sensitivity in distinguishing invasive tumors from intracardiac thrombi [17]. Cardiac metastatic lesions can be identified by their characteristic imaging features: hypo intensity on T1-weighted imaging, hyperintensity on T2-weighted imaging, and diffuse enhancement on late gadolinium enhancement (LGE) sequences. This significantly compensates for the limitation of CT in soft-tissue resolution. Additionally, cardiac MRI can measure key functional parameters such as left ventricular ejection fraction (LVEF), right ventricular ejection fraction (RVEF), and stroke volume. This is of great importance for cardiac function assessment, enabling timely detection of myocardial damage caused by metastatic lesions or pharmacotherapy [19]. Studies have shown that the diagnosis of cardiac masses via cardiac MRI exhibits good consistency with final pathological results [20]. Although pathological diagnosis is the standard method used, surgical biopsy carries a relatively high risk, and postoperative recovery can delay the treatment of the primary lung tumor. Therefore, we opted to guide the patient’s subsequent treatment based on the cardiac MRI diagnosis. Therefore, in clinical practice, PET-CT is often combined with cardiac MRI to improve diagnostic specificity [21].
At present, there is no standardized treatment guideline for lung cancer with cardiac metastasis. Clinical treatment is still based on systemic treatment of the primary tumor. Local treatments such as radiotherapy and radiofrequency ablation can play an auxiliary role. In a reported case of a patient with lung cancer complicated by cardiac metastases and arrhythmia who received stereotactic body radiation therapy (SBRT), the cardiac metastatic lesions were successfully eradicated. Moreover, at 9 months after SBRT and 18 months after the diagnosis of cardiac metastasis, the patient showed no signs of local recurrence, no atrioventricular block, no recurrence of ventricular tachycardia (VT), and required no specific anti-tumor treatment [15]. In our case, the patient had no clinical symptoms at diagnosis. However, the primary lung lesion exhibited a high degree of malignancy, and lymph node metastasis was suspected. Therefore, we prioritized systemic therapy for the primary lesion. From the treatment outcomes, systemic therapy also exerted an inhibitory effect on the cardiac metastatic lesions. In the future, if the myocardial metastatic lesions show persistent activity or induce cardiovascular events, we may consider radiotherapy for these lesions to achieve a better therapeutic effect.
Conclusions
Pulmonary adenocarcinoma complicated with myocardial metastasis is extremely rare in clinical practice. For solid tumors, we strongly recommend completing a PET-CT examination to screen for distant metastatic lesions. When myocardial lesions are detected, cardiac MRI is the most appropriate diagnostic method other than pathological biopsy. It can well compensate for PET-CT’s limitation in distinguishing benign from malignant soft-tissue lesions. With the advancement of imaging examinations, we should not wait for obvious clinical symptoms to occur before implementing intervention measures. Predictive screening can prevent or delay the occurrence of malignant clinical events. In terms of treatment, systemic therapy targeting the primary lesion should be the mainstay, supplemented by local treatments such as radiotherapy and radiofrequency ablation. Given the low incidence of this condition, future efforts should focus on screening high-risk patients and conducting research on individualized treatment regimens.
Figures
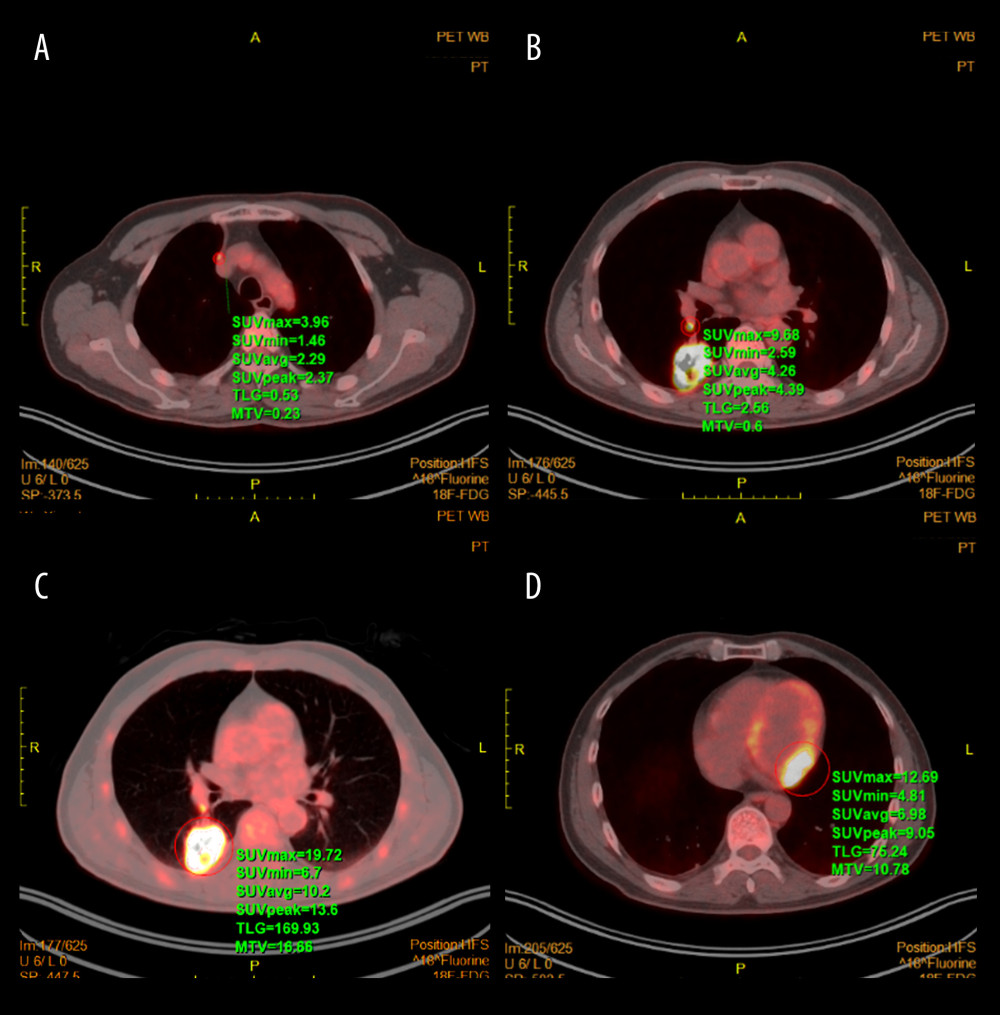 Figure 1. PET-CT images. (A) Mediastinal lymph nodes; (B) Hilar lymph nodes; (C) Adenocarcinoma of the right lower lung lobe; (D) Myocardial metastases in the left ventricle.
Figure 1. PET-CT images. (A) Mediastinal lymph nodes; (B) Hilar lymph nodes; (C) Adenocarcinoma of the right lower lung lobe; (D) Myocardial metastases in the left ventricle. 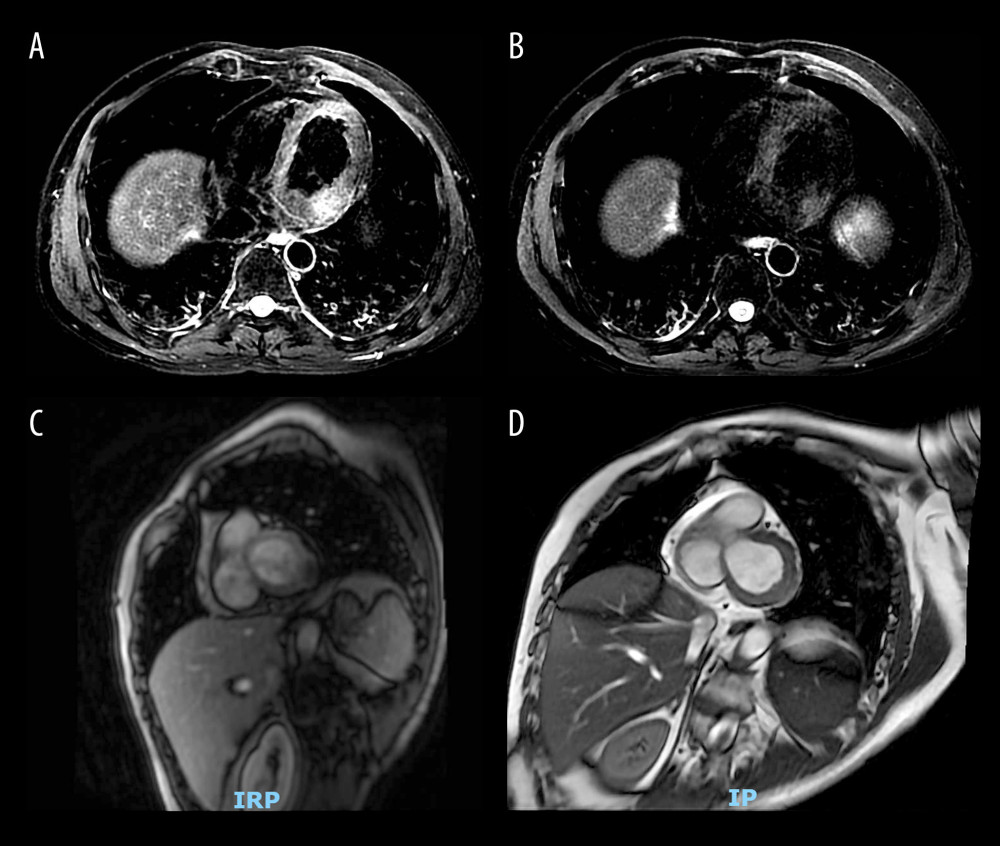 Figure 2. Cardiac MRI images. (A, C) Myocardial metastases before treatment; (B, D) Myocardial metastases after treatment.
Figure 2. Cardiac MRI images. (A, C) Myocardial metastases before treatment; (B, D) Myocardial metastases after treatment. References
1. Al-Mamgani A, Baartman L, Baaijens M, Cardiac metastases: Int J Clin Oncol, 2008; 13(4); 369-72
2. Burazor I, Aviel-Ronen S, Imazio M, Metastatic cardiac tumors: From clinical presentation through diagnosis to treatment: BMC Cancer, 2018; 18(1); 202
3. Di Bari N, D’Errico Ramirez A, Nasso G, Primary malignant cardiac tumors: Sex-related therapy and multidisciplinary approach as a new challenge for the future: J Card Surg, 2022; 37(5); 1287-89
4. Balinski AM, Vasbinder AL, Kerndt CC, Metastatic melanoma of the heart: Retrospective cohort study and systematic review of prevalence, clinical characteristics, and outcomes: Cancer Med, 2023; 12(3); 2356-67
5. Chiles C, Woodard PK, Gutierrez FR, Link KM, Metastatic involvement of the heart and pericardium: CT and MR imaging: Radiographics, 2001; 21(2); 439-49
6. Abe S, Watanabe N, Ogura S, Myocardial metastasis from primary lung cancer: Myocardial infarction-like ECG changes and pathologic findings: Jpn J Med, 1991; 30(3); 213-18
7. Zhao X, Qi Z, Gao Z, He H, High counting of circulating tumor cells in blood is not directly related to metastasis: Cytometry A, 2023; 103(1); 82-87
8. Bussani R, Castrichini M, Restivo L, Cardiac tumors: Diagnosis, prognosis, and treatment: Curr Cardiol Rep, 2020; 22(12); 169
9. Pohar S, Bhandari J, Chaudhuri D, Rare cardiac metastasis of lung cancer mimicking aneurysm and tamponade: Proc (Bayl Univ Med Cent), 2024; 37(5); 866-69
10. Kunishige R, Matsuoka Y, Yoshimura R, Cardiac metastasis of lung cancer presented as mimicking ST-elevation myocardial infarction with reciprocal electrocardiographic changes: J Cardiol Cases, 2022; 26(3); 173-77
11. Zhou J, Zhan C, Zhou J, Case report: Persistent ST-segment elevation due to cardiac metastasis from lung cancer: Front Cardiovasc Med, 2023; 10; 1001527
12. Ritter A, Quartermaine C, Pierre-Charles J, Cardiotoxicity of anti-cancer radiation therapy: A focus on heart failure: Curr Heart Fail Rep, 2023; 20(1); 44-55
13. Zhang X, Gao Y, Yang B, The mechanism and treatment of targeted anti-tumour drugs induced cardiotoxicity: Int Immunopharmacol, 2023; 117; 109895
14. Wang S, Zhao J, Wang C, Zhang N, Prognosis and role of clinical and imaging features in patients with malignant pericardial effusion: A single-center study in China: BMC Cardiovasc Disord, 2021; 21(1); 565
15. Jumeau R, Vincenti MG, Pruvot E, Curative management of a cardiac metastasis from lung cancer revealed by an electrical storm: Clin Transl Radiat Oncol, 2020; 21; 62-65
16. Shi Y, Duan S, Zhang L, A primary benign cardiac tumor misdiagnosed as cardiac metastasis in the right atrium: Echocardiography, 2020; 37(10); 1678-81
17. Lichtenberger JP, Reynolds DA, Keung J, Metastasis to the heart: A radiologic approach to diagnosis with pathologic correlation: Am J Roentgenol, 2016; 207(4); 764-72
18. Dilsizian V, 18F-FDG uptake as a surrogate marker for antecedent ischemia: J Nucl Med, 2008; 49(12); 1909-11
19. Rajiah PS, François CJ, Leiner T, Cardiac MRI: State of the art: Radiology, 2023; 307(3); e223008
20. Tonso S, Castillo SD, Garagoli F, Assessment of cardiac masses by magnetic resonance imaging: Prognostic value and agreement with histopathology: Curr Probl Cardiol, 2025; 50(8); 103084
21. Bilani N, Elson L, Martinez F, A multimodal approach to evaluate for cardiac metastasis in a case of non-small cell lung cancer: Case Rep Oncol, 2020; 13(1); 212-18
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133