27 December 2025: Articles 
ANCA-Negative Eosinophilic Granulomatosis With Polyangiitis Presenting With Duodenal Stenosis: A Case Report
Rare disease
Jiajia Chen AF 1, Jiajun Liu BCD 2, Min Luo DF 3, Jiguang Guo ACE 3*DOI: 10.12659/AJCR.951493
Am J Case Rep 2025; 26:e951493






Abstract
BACKGROUND: Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare ANCA-associated vasculitis characterized by asthma, eosinophilia, and multi-organ involvement. Duodenal stenosis is an uncommon gastrointestinal complication, with few reported cases linked to EGPA.
CASE REPORT: A 71-year-old man with a 2-week history of recurrent abdominal distension and pain was admitted to our hospital. Notably, there was a marked elevation in absolute eosinophil count (1.13×10⁹/L) and eosinophils (14.3%), while ANCA was negative. Additionally, elevated levels of erythrocyte sedimentation rate and C-reactive protein were observed. Electronic gastroscopy revealed duodenal bulb stenosis, with pathological findings indicating significant eosinophil infiltration. The patient, with a history of asthma, exhibited neurological impairment symptoms alongside elevated eosinophil levels. After excluding parasitic infections, hypereosinophilic syndrome, and eosinophilic gastroenteritis based on systemic involvement and diagnostic criteria, EGPA was considered as the diagnosis. Following treatment with methylprednisolone (0.8 mg/kg/day) and cyclophosphamide (5 mg/kg IV every 2 weeks), the patient experienced substantial relief in abdominal distension and pain symptoms. Concurrently, parameters including eosinophil count, C-reactive protein level, and erythrocyte sedimentation rate progressively normalized. The 4-month follow-up gastroscopy showed significant improvement of duodenal stenosis.
CONCLUSIONS: Duodenal stenosis is a rare but serious manifestation of EGPA, likely resulting from eosinophilic infiltration and inflammation. This case highlights the need to consider EGPA in asthmatic patients presenting with gastrointestinal obstruction and eosinophilia. Early immunosuppressive therapy can improve outcomes, and endoscopic evaluation remains essential. Even without classic vasculitic histology, EGPA can be diagnosed based on systemic criteria, with gastrointestinal obstruction as a potential initial manifestation.
Keywords: Duodenum, Vasculitis, Eosinophilia, Humans, Male, Aged, Antibodies, Antineutrophil Cytoplasmic, Duodenal Obstruction, Churg-Strauss syndrome, granulomatosis with polyangiitis
Introduction
Eosinophilic granulomatosis with polyangiitis (EGPA), previously referred to as Churg-Strauss syndrome, is an antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis primarily affecting small- to medium-sized blood vessels. It is pathologically characterized by eosinophil-rich tissue infiltration, necrotizing vasculitis, and granulomatous inflammation. Unlike the other 2 types of ANCA-associated vasculitis (granulomatosis with polyangiitis and microscopic polyangiitis), EGPA is characterized by asthma, sinusitis, eosinophilia, and eosinophil infiltration in tissues and blood [1]. Gastrointestinal involvement is reported in approximately 20% to 30% of patients with EGPA and is associated with significant morbidity and a poorer prognosis [2]. Duodenal stenosis is frequently attributed to ulcers, Crohn disease, and tumors. However, when associated with eosinophilia, eosinophilic gastroenteritis (EGID) is the most common cause. Duodenal stenosis as a direct manifestation of EGPA is exceptionally rare, with limited documentation on the combination of EGPA and duodenal stenosis. In this case report, we describe a unique presentation of ANCA-negative EGPA manifesting as duodenal stenosis, underscoring the diagnostic challenges and the importance of a multidisciplinary approach.
Case Report
ADDITIONAL DIAGNOSTIC WORKUP:
Endoscopic examination revealed deformation and edema in the duodenal bulb, accompanied by stenosis at the junction of the duodenal bulb and its descending portion (Figure 1). Pathological examination of the duodenal bulb indicated extensive eosinophil infiltration (>20 eosinophils per high-power field in the mucosal layer; Figure 2). The biopsy was limited to the mucosa and submucosa; no vasculitis or granulomas were identified in the sampled tissue. Bilateral pure tone audiometry indicated sensorineural hearing loss (primarily in the high frequencies, mild to moderate in degree), with normal middle ear transmission function. A chest computed tomography (CT) scan showed emphysema accompanied by local nodular thickening of the pleura. A sinus CT scan revealed mild mucosal thickening in the maxillary sinuses. Nerve conduction studies and fundus examination were offered, but the patient declined. Laboratory test results indicated an increase in the proportion of eosinophils (14.3%) and absolute eosinophil count (1.13×109/L), as well as increased levels of erythrocyte sedimentation rate (ESR, 90 mm/h), C-reactive protein (CRP, 32.5 mg/L), and ANA titer (1: 100). Laboratory investigations revealed an elevated total IgE level of 450 IU/mL. Stool examination for ova and parasites was negative, and serological tests for common parasites (eg, Strongyloides) were also negative. Urinalysis showed no proteinuria or active sediment. The serum creatinine level was within the reference range. Cardiac evaluation included a normal troponin I level, NT-proBNP level, and echocardiogram. Both the cytoplasmic ANCA and perinuclear ANCA tests were negative. The remaining laboratory test results and the dynamic changes in ESR, CRP, and eosinophil counts are presented in Table 1 and Figure 3. On admission, vital signs were as follows: blood pressure of 128/73 mmHg, pulse rate of 82 beats/min, respiratory rate of 18 breaths/min, and body temperature of 36.7°C. Physical examination revealed mild tenderness in the upper abdomen and decreased breath sounds in both lungs.
DIFFERENTIAL DIAGNOSIS:
The differential diagnosis for eosinophilia with gastrointestinal obstruction included parasitic infection, hypereosinophilic syndrome (HES), and EGID. The absence of travel history, negative stool and serology tests, and the presence of systemic features (asthma, sinusitis, neuropathy) provided evidence against parasitic infection. The lack of a clonal hematopoietic disorder and the presence of asthma and vasculitic features (although not histologically confirmed) made HES less likely. While EGID can cause transmural eosinophilic infiltration and stenosis, the combination with extra-intestinal manifestations such as neuropathy and a long-standing history of asthma strongly favored the diagnosis of EGPA.
The patient presented with elevated eosinophil levels and symptoms of neurological impairment. Pathological findings from the duodenal bulb revealed significant eosinophilic infiltration. Considering these findings and the patient’s history of asthma, and based on the 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria [3], a diagnosis of EGPA was established.
Following assessment of the poor prognostic factors using the five-factor score [4], the patient was treated with methylprednisolone tablets (0.8 mg/kg, orally, once daily, reduced dosage after 2 months) and cyclophosphamide (5 mg/kg, IV infusion every 2 weeks, a total of 3 months of treatment) during the induction remission phase. Subsequently, after 3 months, cyclophosphamide was replaced with mycophenolate mofetil (0.5 g, orally, twice daily) during the maintenance remission phase. Considering the patient’s history of hepatitis B and the use of immunosuppressive medications, entecavir (0.5 mg, orally, once daily) was administered for antiviral treatment. In addition, concomitant routine medications included calcium carbonate (0.6 g, orally, once daily) and omeprazole enteric-coated capsules (20 mg, orally, once daily). Prophylaxis against Pneumocystis jirovecii pneumonia with trimethoprim-sulfamethoxazole was also initiated.
At the 4-month follow-up, the patient experienced significant alleviation of abdominal distension and pain, with no reported joint pain. In addition, the peripheral blood eosinophil percentage, ESR, and CRP levels in this patient remained within the reference ranges. Follow-up gastroscopy performed at an external hospital in another city revealed marked improvement in duodenal bulb edema and luminal patency, with only mild residual deformity observed.
Discussion
EGPA VS EGID:
A key diagnostic challenge in this case was distinguishing EGPA from EGID, as both can cause significant eosinophilic infiltration of the gastrointestinal tract, leading to stenosis. EGID is primarily a disorder confined to the gastrointestinal tract, although rare extra-intestinal manifestations can occur. The diagnosis of EGID requires the exclusion of other causes of eosinophilia, including EGPA. Our patient’s well-established history of asthma, the presence of sensorineural hearing loss (suggesting extra-intestinal organ involvement), and sinusitis are features that are not typical of EGID and are core components of the EGPA classification criteria. Therefore, despite the absence of vasculitis on the superficial mucosal biopsy, the constellation of systemic findings firmly supports EGPA as the unifying diagnosis.
Moreover, there have been limited reports of EGPA cases involving the gastrointestinal system. Yagi et al reported the first case of EGPA-like vasculitis in a child presenting with acute pancreatitis, revealing marked eosinophil infiltration in the pancreas upon autopsy [7]. Ye et al reported multiple cases of cholecystitis complicated with EGPA through pathological examination of resected gallbladders. Among these patients, 91.7% exhibited favorable responses to steroid and immunosuppressant therapies [8]. In patients with eosinophilic gastrointestinal diseases, eosinophilic infiltration of the muscular layer of the intestine can lead to local tissue edema and fibrosis, ultimately resulting in intestinal stenosis and obstruction [9]. Gastroscopy revealed local edema and stenosis in the duodenal bulb of our patient. These findings suggest a strong association with extensive eosinophil infiltration. The clinical and endoscopic response to immunosuppressive therapy further supports an inflammatory, EGPA-related etiology.
The treatment of EGPA remains somewhat controversial, mainly depending on factors such as disease severity, organ involvement, and disease activity. The conventional treatment regimen for EGPA relies on systemic corticosteroids combined with immunosuppressants for severe or refractory diseases. Recent research has highlighted the potential role of inerleukin (IL)-5, a critical factor in eosinophil activation, in the pathogenesis of EGPA. IL-5 not only induces the differentiation and maturation of eosinophils but also inhibits their apoptosis [10]. Mepolizumab, the first drug developed and approved for the treatment of severe eosinophilic asthma, functions by inhibiting IL-5-related signal transduction in eosinophils, thereby impeding their activation and tissue accumulation. Recent international guidelines, including the 2024 EULAR updates, reinforce this approach for severe cases [11]. A double-blind, randomized, placebo-controlled trial conducted in 2017 demonstrated that mepolizumab notably extended the duration of remission in patients with EGPA, with a higher proportion of individuals achieving remission. Additionally, mepolizumab facilitates a reduction in glucocorticoid dosage [12]. Another study showed that the reduction in the use of oral corticosteroids was greater in the mepolizumab-treated group, compared with the placebo group. Moreover, regardless of whether patients with EGPA have previously used immunosuppressants, or the length of the EGPA disease course, mepolizumab can provide clinical benefits [13]. In the present case, a combination of corticosteroids and cyclophosphamide was administered for the treatment of EGPA complicated by duodenal stenosis, resulting in a favorable therapeutic outcome. The patient’s symptoms of abdominal distension and pain were significantly alleviated, and disease activity was effectively controlled.
Conclusions
This case of ANCA-negative EGPA presenting with duodenal stenosis highlights a rare but significant gastrointestinal manifestation of the disease, likely driven by intense eosinophilic infiltration leading to tissue edema and fibrotic stenosis. While the superficial biopsies did not demonstrate vasculitis, the diagnosis was confirmed by fulfilling recognized classification criteria based on clinical features. We hypothesize that in ANCA-negative EGPA, dense eosinophilic infiltration may preferentially affect the gastrointestinal muscular layer, leading to obstructive complications; however, this observation from a single case requires validation in larger cohorts, as the generalizability of these observations is limited by the nature of a single case report. We recommend that EGPA be considered in the differential diagnosis for patients with a history of asthma or chronic respiratory disease who present with eosinophilia and unexplained gastrointestinal symptoms, such as obstruction, pancreatitis, or cholecystitis. Further cohort studies are needed to validate these recommendations.
Figures
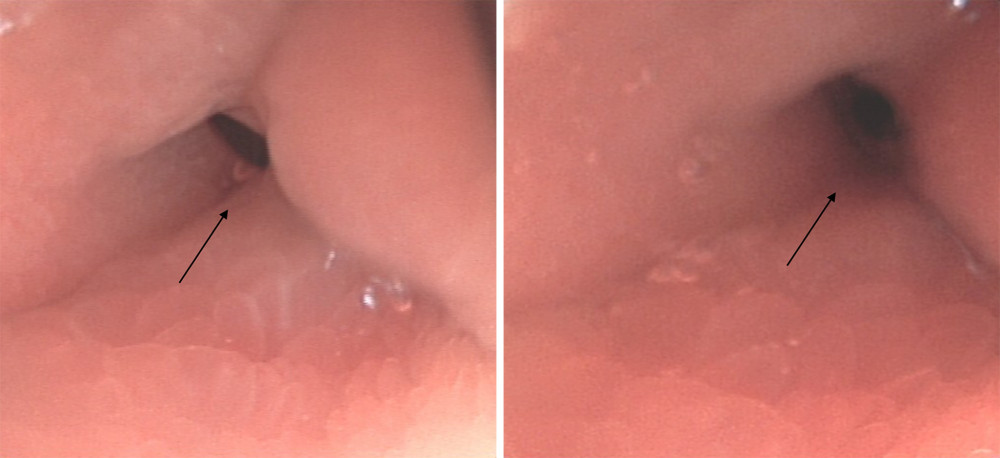 Figure 1. Electronic gastroscopy reveals deformation of the duodenal bulb, with stenosis observed at the junction of the duodenal bulb and its descending portion. The black arrow indicates stenosis at the junction of the duodenal bulb and the descending part of the duodenum.
Figure 1. Electronic gastroscopy reveals deformation of the duodenal bulb, with stenosis observed at the junction of the duodenal bulb and its descending portion. The black arrow indicates stenosis at the junction of the duodenal bulb and the descending part of the duodenum. 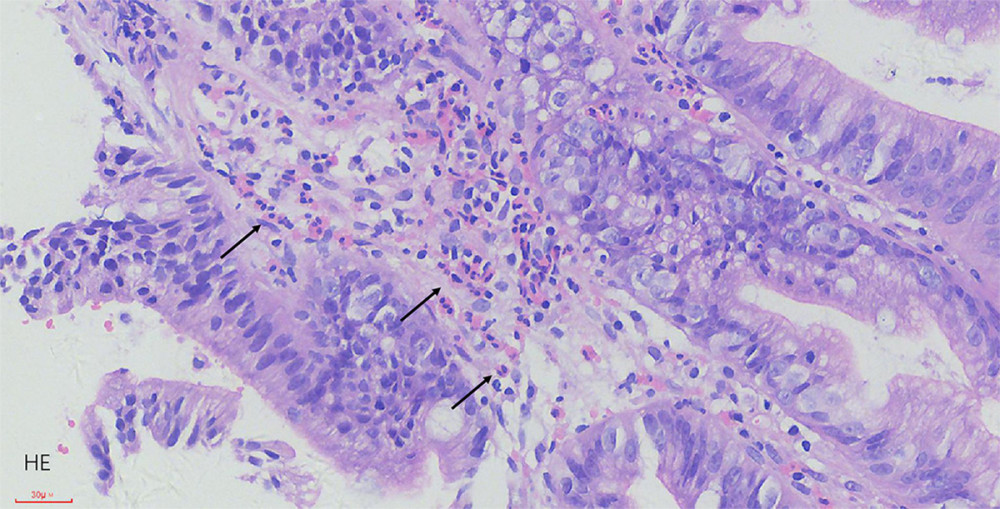 Figure 2. The pathological results indicate extensive infiltration of eosinophils in the duodenal bulb. The black arrow indicates eosinophils.
Figure 2. The pathological results indicate extensive infiltration of eosinophils in the duodenal bulb. The black arrow indicates eosinophils. 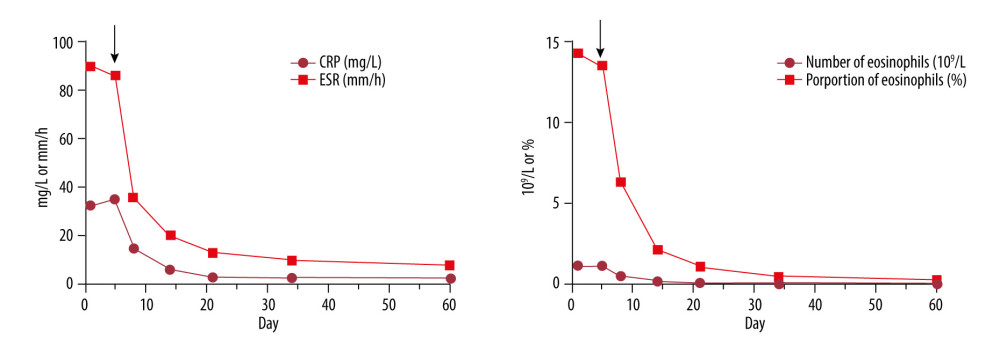 Figure 3. Dynamic changes in erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and eosinophils during the treatment. The black arrows indicate the day of glucocorticoid and cyclophosphamide therapy.
Figure 3. Dynamic changes in erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and eosinophils during the treatment. The black arrows indicate the day of glucocorticoid and cyclophosphamide therapy. 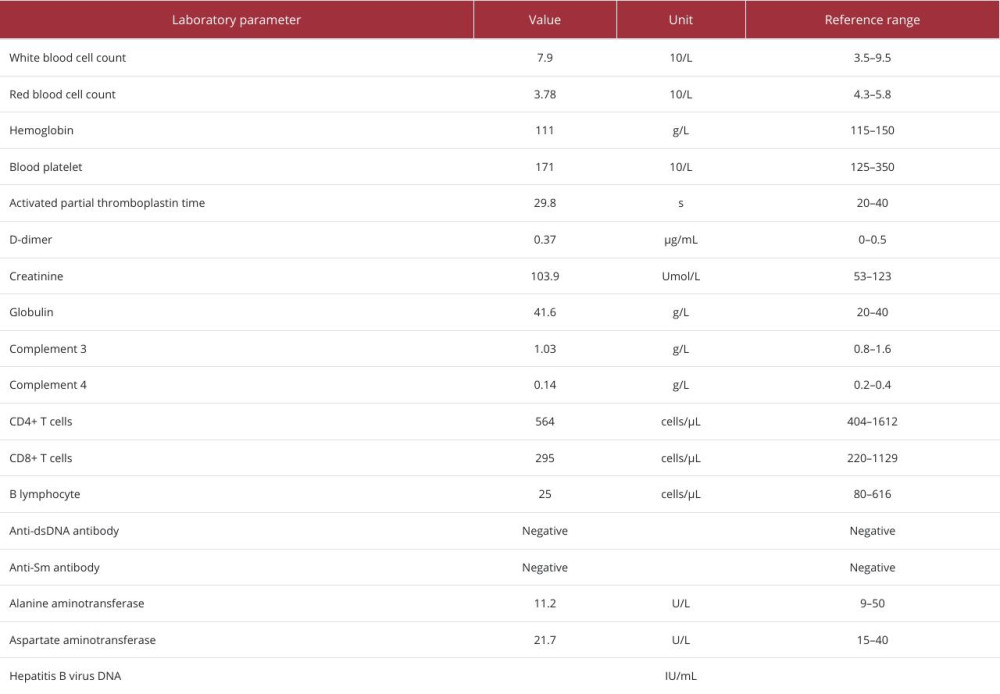
References
1. Cottin V, Bel E, Bottero Pthe Groupe d’Etudes et de Recherche sur les Maladies Orphelines Pulmonaires (GERM“O”P), Respiratory manifestations of eosinophilic granulomatosis with polyangiitis (Churg-Strauss): Eur Respir J, 2016; 48(5); 1429-41
2. Comarmond C, Pagnoux C, Khellaf MFrench Vasculitis Study Group, Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): Clinical characteristics and long-term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort: Arthritis Rheum, 2013; 65(1); 270-81
3. Grayson PC, Ponte C, Suppiah RDCVAS Study Group, 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis: Ann Rheum Dis, 2022; 81(3); 309-14
4. Nguyen Y, Guillevin L, Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): Semin Respir Crit Care Med, 2018; 39(4); 471-81
5. Trivioli G, Terrier B, Vaglio A, Eosinophilic granulomatosis with polyangiitis: Understanding the disease and its management: Rheumatology (Oxford), 2020; 59(Suppl 3); iii84-iii94
6. Nishi R, Koike H, Ohyama K, Differential clinicopathologic features of EGPA-associated neuropathy with and without ANCA: Neurology, 2020; 94(16); e1726-e37
7. Yagi H, Takahashi S, Kibe T, An autopsy case of a 5-year-old child with acute pancreatitis caused by eosinophilic granulomatosis with polyangiitis-like necrotizing vasculitis: Case Rep Rheumatol, 2019; 2019; 9053747
8. Ye L, Lu X, Xue J, Eosinophilic granulomatosis with polyangiitis complicated by cholecystitis: a case report and review of the literature: Clin Rheumatol, 2016; 35(1); 259-63
9. Yun MY, Cho YU, Park IS, Eosinophilic gastroenteritis presenting as small bowel obstruction: A case report and review of the literature: World J Gastroenterol, 2007; 13(11); 1758-60
10. Furuta S, Iwamoto T, Nakajima H, Update on eosinophilic granulomatosis with polyangiitis: Allergol Int, 2019; 68(4); 430-36
11. Hellmich B, Sanchez-Alamo B, Schirmer JH, EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update: Ann Rheum Dis, 2024; 83(1); 30-47
12. Wechsler ME, Akuthota P, Jayne DEGPA Mepolizumab Study Team, Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis: N Engl J Med, 2017; 376(20); 1921-32
13. Jayne DRW, Terrier B, Hellmich B, Mepolizumab has clinical benefits including oral corticosteroid sparing irrespective of baseline EGPA characteristics: ERJ Open Res, 2024; 10(1); 00509-2023
Figures
Figure 1. Electronic gastroscopy reveals deformation of the duodenal bulb, with stenosis observed at the junction of the duodenal bulb and its descending portion. The black arrow indicates stenosis at the junction of the duodenal bulb and the descending part of the duodenum.Figure 2. The pathological results indicate extensive infiltration of eosinophils in the duodenal bulb. The black arrow indicates eosinophils.Figure 3. Dynamic changes in erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and eosinophils during the treatment. The black arrows indicate the day of glucocorticoid and cyclophosphamide therapy. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133