30 December 2025: Articles 
Atrial Septal Defect Patch Closure From the Left Atrial Side Approach in Totally Endoscopic Minimally Invasive Cardiac Surgery: A Case Report
Unusual setting of medical care
Shizuya Shintomi ABCDEF 1*, Takashi Oshitomi ABCD 1, Kenetaro Takaji A 1, Shigeru Okada B 1, Katsuyuki Shigehara A 1, Ichiro Ideta A 1, Hideyuki Uesugi A 1DOI: 10.12659/AJCR.951594
Am J Case Rep 2025; 26:e951594






Abstract
BACKGROUND: Transcatheter atrial septal defect closure is currently the standard approach. In addition, minimally invasive cardiac surgery is preferable over median sternotomy. However, ensuring safe and reliable surgery is essential. The conventional right atrial approach is limited in its ability to ensure a clear surgical field and is associated with bleeding and postoperative arrhythmia. Herein, we describe atrial septal defect patch closure using a left atrial side approach in totally endoscopic minimally invasive cardiac surgery.
CASE REPORT: A 61-year-old man was admitted for heart failure caused by atrial fibrillation. Echocardiography revealed an atrial septal defect (27×17 mm; Qp/Qs ratio, 2.5). Given the relatively small aortic rim (1 mm), surgery after ablation of atrial fibrillation was selected. Complete pulmonary vein antrum isolation was performed using a catheter, followed by confirming sinus rhythm restoration. Two years later, the patient underwent atrial septal defect closure in a totally endoscopic minimally invasive cardiac surgery via the right axillary mini-thoracotomy under moderate hypothermia. The defect was accessed using a standard right-sided left atrial incision; brief circulatory arrest allowed secure suturing of the lower defect margin adjacent to the inferior vena cava, with minimal blood loss. The patient had an uneventful recovery. Postoperative echocardiography confirmed complete closure without residual shunting.
CONCLUSIONS: Compared with conventional right atriotomy, the left atrial side approach provided improved exposure, reduced bleeding, and easier air evacuation, potentially lowering the risk of long-term arrhythmias. This technique could offer a familiar and useful approach for enhancing the safety of atrial septal defect closures.
Keywords: Atrial Fibrillation, Atrial Septum, Minimally Invasive Surgical Procedures, Humans, Male, Middle Aged, Heart Septal Defects, Atrial, Cardiac Surgical Procedures, endoscopy, Heart Atria
Introduction
With transcatheter atrial septal defect (ASD) closure currently established as the standard minimally invasive treatment, surgical intervention should preferably be performed using minimally invasive cardiac surgery (MICS) rather than median sternotomy. However, ensuring that MICS for ASD closure is safely and reliably performed is essential. Although MICS for ASD closure has demonstrated reliable outcomes [1], the conventional right atrial approach has certain limitations in total endoscopic MICS. Specifically, these include constraints on surgical field traction due to the distance from the anterior chest, suture hole bleeding from the thin-walled atrial incision, and postoperative atrial arrhythmias. To address these challenges, our institution adopted the novel technique of ASD patch closure from the left atrial side approach in totally endoscopic MICS. This case report describes the high efficacy of this novel technique.
Case Report
A 61-year-old man (height, 178 cm; weight, 69 kg; body surface area, 1.85 m2) was admitted to our hospital for heart failure due to atrial fibrillation. Echocardiography and computed tomography revealed an ASD (27×17 mm; Qp/Qs ratio, 2.5; Figures 1–4). Complete pulmonary vein antrum isolation using a catheter was first performed, after which sinus rhythm restoration was confirmed. Two years later, surgical ASD closure was chosen over transcatheter ASD closure owing to the small aortic rim diameter of 1 mm.
The patient underwent ASD closure in totally endoscopic MICS under general anesthesia with differential lung ventilation in a partially left lateral position (Video 1). A right axillary mini-thoracotomy was performed with a 3-cm vertical skin incision in the fourth intercostal space. The main incision was enlarged using a wound protector. Three additional ports were placed at the third, fourth, and fifth intercostal spaces. We filled the thoracic cavity with CO2, and the intervention was performed under moderate hypothermia (28°C). Cardiopulmonary bypass was initiated via femoral arterial and venous cannulation, as well as percutaneous superior vena cava cannulation via the right jugular vein. The pericardium, subsequently, was vertically incised. The left atrial appendage resection was performed via the transverse sinus using a stapler. The cardioplegia was applied through a root cannula after clamping of the ascending aorta. The superior vena cava was clamped; thereafter, a standard right-sided left atrium incision was made through the Waterstone’s groove to expose the ASD from the left atrial side. After opening the left atrium, the central portion of the posterior septal margin was elevated using a 4-0 polypropylene mattress suture with a felt pledget. This was done to prevent the atrial septum from slipping off the retractor when securing the ASD field of view, owing to absence of an atrial septal wall. The fabric sheet (Cardiovascular Fabrics; Becton, Dickinson and Company, Franklin Lakes, NJ, USA) was trimmed and initially sutured to the aortic margin of the atrial septum using a 4-0 polypropylene suture in a continuous pattern (Figure 5). To avoid atrioventricular block, the left atrial side of the septal wall was sutured in this area. The venous blood leakage from the inferior vena cavasuperior vena cava (IVC) cannula could obscure the field during suturing of the lower edge of the ASD near the IVC. Therefore, the circulatory arrest of 2 to 3 min was used exclusively for suturing this area. After the ASD closure, the leakage could be confirmed by filling the right atrium. The IVC cannula tip, which was in the IVC, was then inserted into the right atrium. The left atrial incision was closed with 4-0 polypropylene continuous sutures from both ends of the incision line, and a vent tube was inserted through the left atrial incision line. Subsequently, the aortic clamp was released. The vent tube and arterial cannula were removed after evacuating air. Hemostasis and weaning from cardiopulmonary bypass were smoothly achieved. The pericardium was completely closed; the total blood loss was 660 mL. The cross-clamp and cardiopulmonary bypass times were 134 and 282 min, respectively.
Postoperatively, the patient’s clinical condition improved (intubation time, 15 hours; mobilization initiation, postoperative day 1; chest tube removal, postoperative day 5; discharged, postoperative day 9). The patient returned to work and made a full recovery. At the outpatient follow-up 2 years postoperatively, echocardiography showed no residual shunt; the patient’s clinical course remained uneventful (Figure 6).
Discussion
Surgical intervention should preferably be performed using MICS rather than median sternotomy to achieve a smaller incision and reduce the risk of sternal osteomyelitis and mediastinitis associated with avoiding sternotomy [2,3]. From an anatomical perspective, the ASD closure typically requires several surgical procedures [4]. Numerous reports have suggested that MICS is effective with consistent quality outcomes. However, the primary concern with MICS is safety, particularly in the ASD closure, as hemostasis depends on proper atriotomy closure. In cases of a dilated right atrium, the atrial muscle is thin, making it prone to bleeding from needle holes. Additionally, once volume is added to the right atrium and the venous pressure rises, achieving hemostasis on the IVC side becomes challenging. Additional disadvantages of a right atriotomy include the short distance from the incision line to the anterior chest wall, making positioning the atrial retractor difficult; the potential to cause supraventricular arrhythmias in the long term; and difficulty in detecting leaks after the ASD closure. Although various modifications to the right atrial approach have been reported, they might be insufficient to fully resolve all associated issues [5].
The left atrial side approach was selected based on several factors. This approach offers cosmetic benefits and advantages in pain control; reduced bleeding; ease in concomitant interventions for left atrial appendage closure, pulmonary vein isolation, and mitral valve surgery via a familiar incision; prevention of long-term supraventricular arrhythmias due to right atriotomy syndrome (particularly in young patients); ample distance to the ceiling of the chest wall provided by the incision line, making air evacuation easier than that with right atriotomy in MICS; and easier and more reliable air removal during left atrial closure. A similar approach was used in 8 cases. The mean age of the cohort, which included 4 male patients, was 51.5±17.1 years. The mean cross-clamp time was 110.6±38.6 minutes, and the mean cardiopulmonary bypass time was 214.4±66.1 minutes. The average blood loss was 923.8±355.8 mL; 4 of the cases were managed without the need for blood transfusion. The mean duration of intubation was 12.5±11.5 hours; chest tube was removed on postoperative day 3.0±2.2; and the average length of hospital stay postoperatively was 11.4±3.7 days. These operations have a learning curve, and cross-clamp and cardiopulmonary bypass times are expected to decrease in the future. In all cases, no residual shunt was observed, and follow-up in the outpatient clinic revealed no complications, with all patients resuming normal daily activities. Compared with the period when the right atrial approach was used, this approach can be safely performed by surgical residents, given the ease of hemostasis and low risk of bleeding.
Although the literature supports the utility of MICS [2,3], to the best of our knowledge, no published studies have reported the routine use of the left atrial side approach for ASD closure. This technique offers a familiar and useful approach for enhancing the safety of the ASD closure.
Conclusions
Compared with conventional right atriotomy, the left atrial side approach provided improved exposure, reduced bleeding, and easier air evacuation, potentially lowering the risk of long-term arrhythmias. This technique could offer a familiar and useful approach for enhancing the safety of ASD closures.
Figures
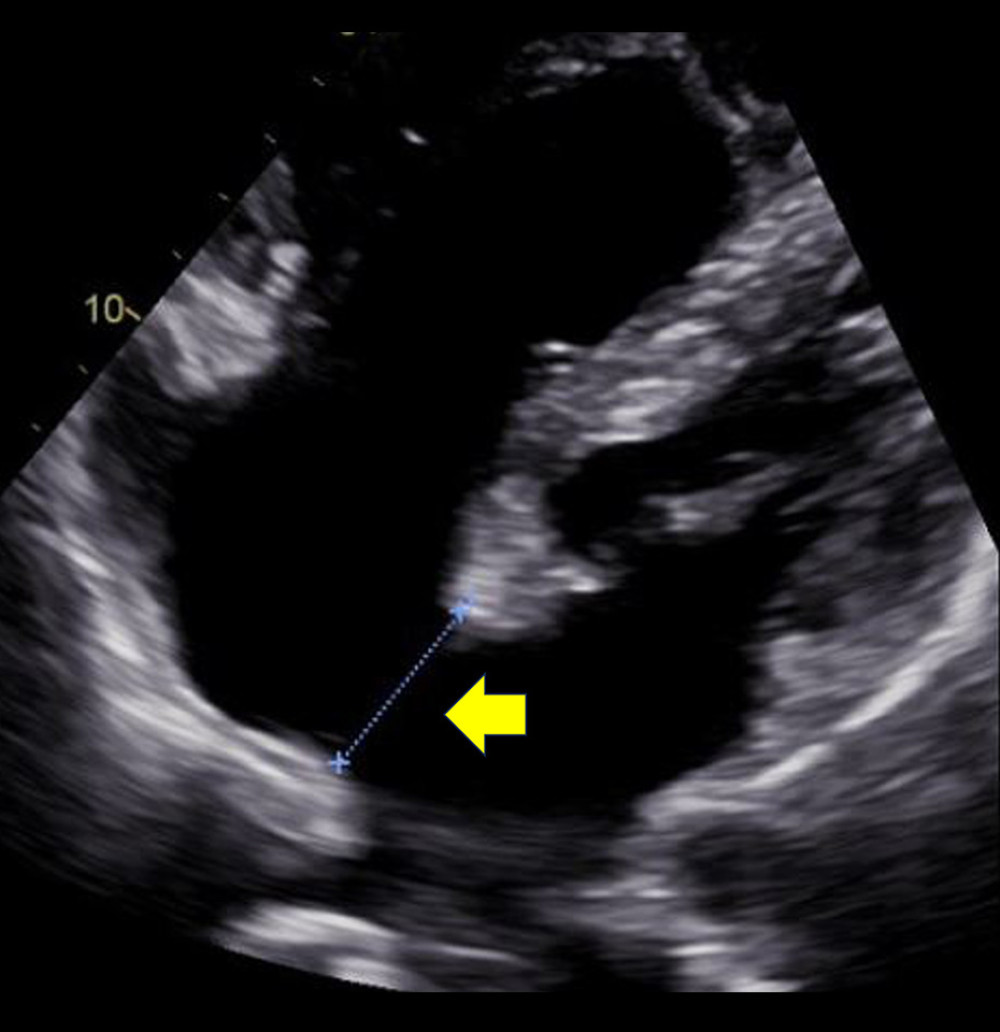 Figure 1. Preoperative transthoracic echocardiography shows an atrial septal defect (yellow arrow).
Figure 1. Preoperative transthoracic echocardiography shows an atrial septal defect (yellow arrow). 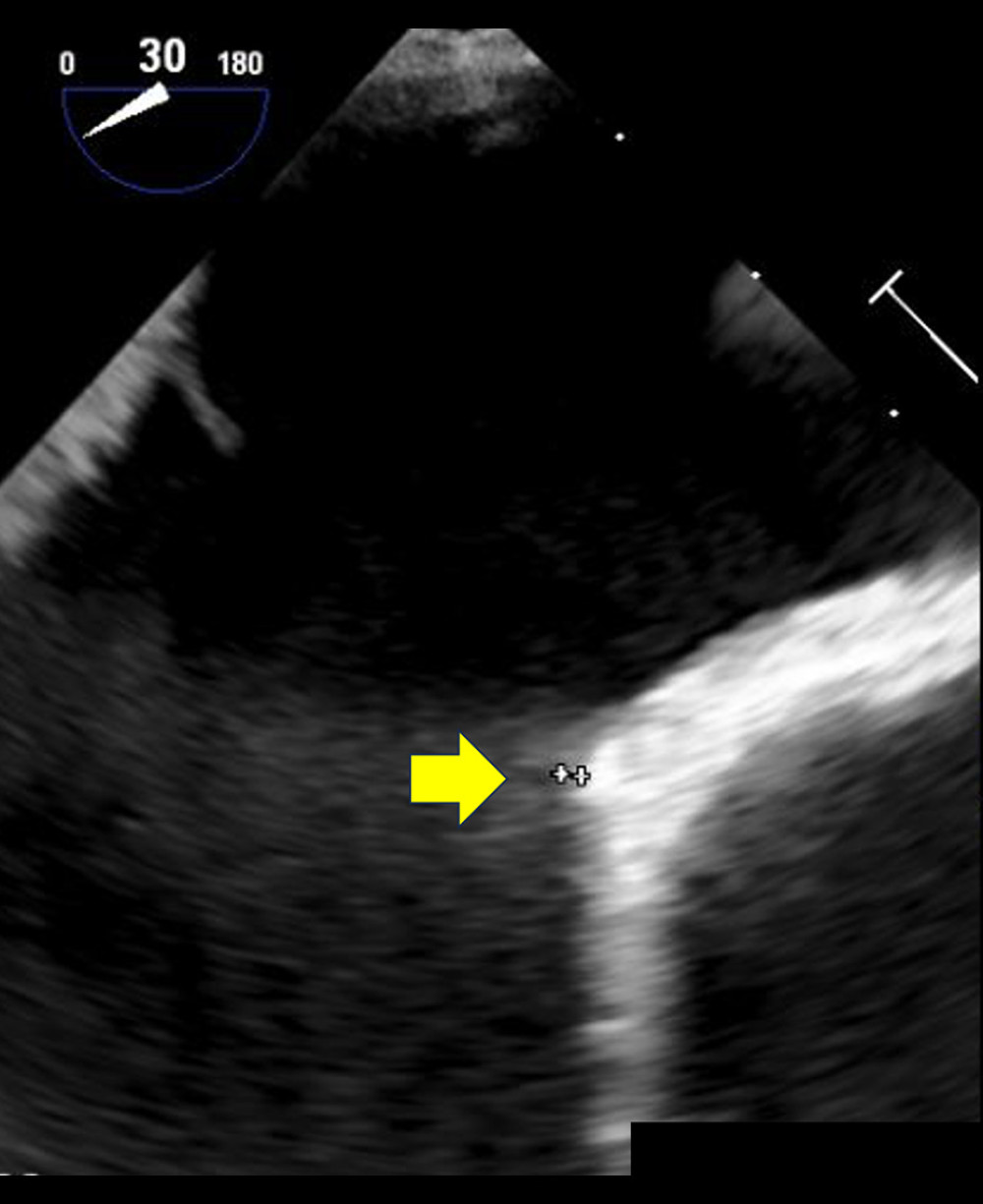 Figure 2. Preoperative transesophageal echocardiography shows a relatively small aortic rim of only 1 mm (yellow arrow).
Figure 2. Preoperative transesophageal echocardiography shows a relatively small aortic rim of only 1 mm (yellow arrow).  Figure 3. Preoperative computed tomography scan shows an atrial septal defect (yellow arrow).
Figure 3. Preoperative computed tomography scan shows an atrial septal defect (yellow arrow). 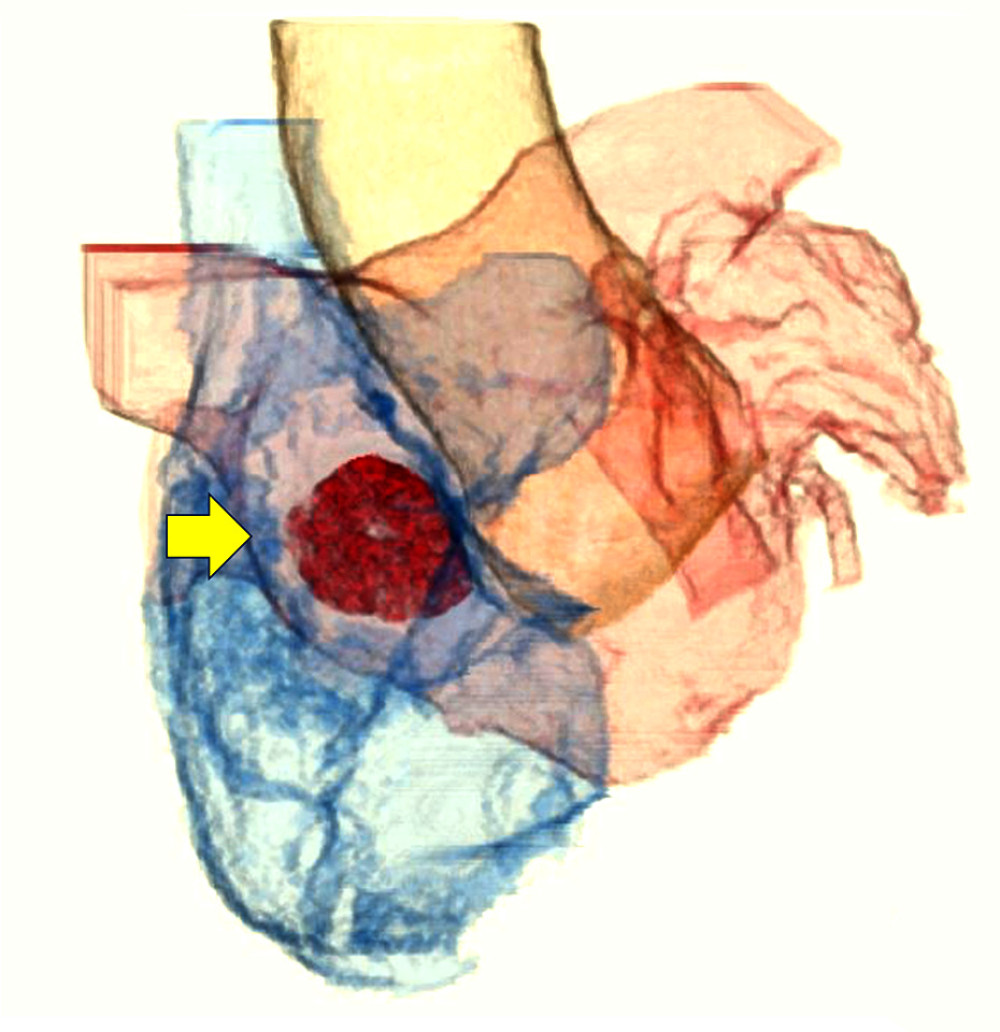 Figure 4. Preoperative computed tomography scan (volume rendering) shows an atrial septal defect (yellow arrow).
Figure 4. Preoperative computed tomography scan (volume rendering) shows an atrial septal defect (yellow arrow). 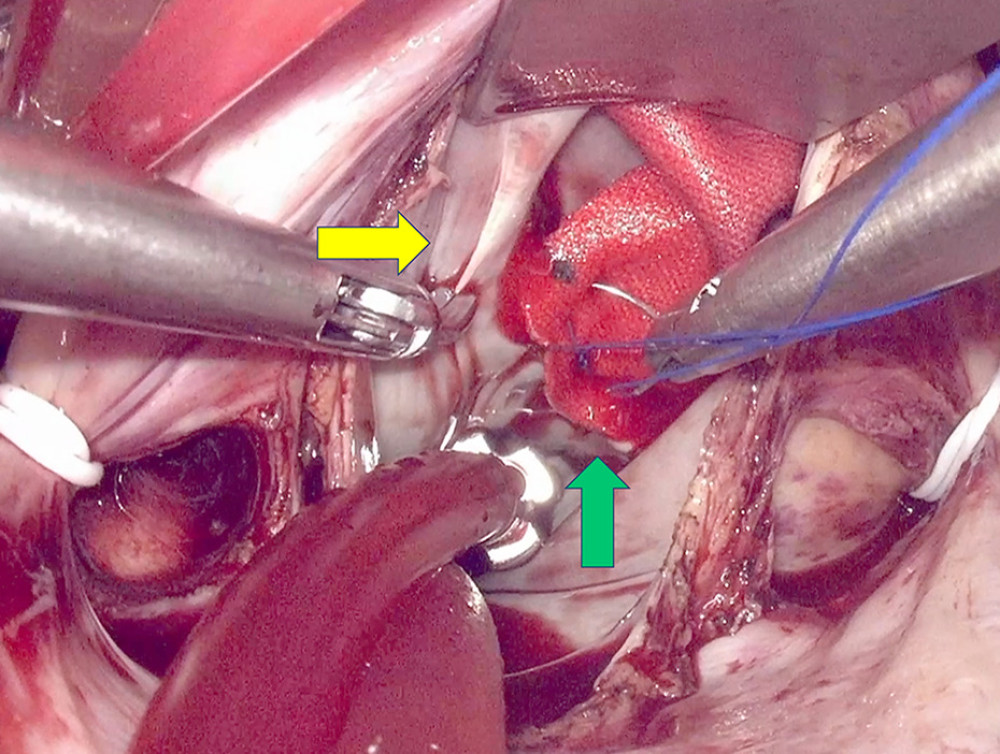 Figure 5. Atrial septal defect patch closure was performed via the left atrial side approach using totally endoscopic minimally invasive cardiac surgery. The yellow arrow indicates the atrial septal defect margin; the green arrow represents the fabric sheet.
Figure 5. Atrial septal defect patch closure was performed via the left atrial side approach using totally endoscopic minimally invasive cardiac surgery. The yellow arrow indicates the atrial septal defect margin; the green arrow represents the fabric sheet. 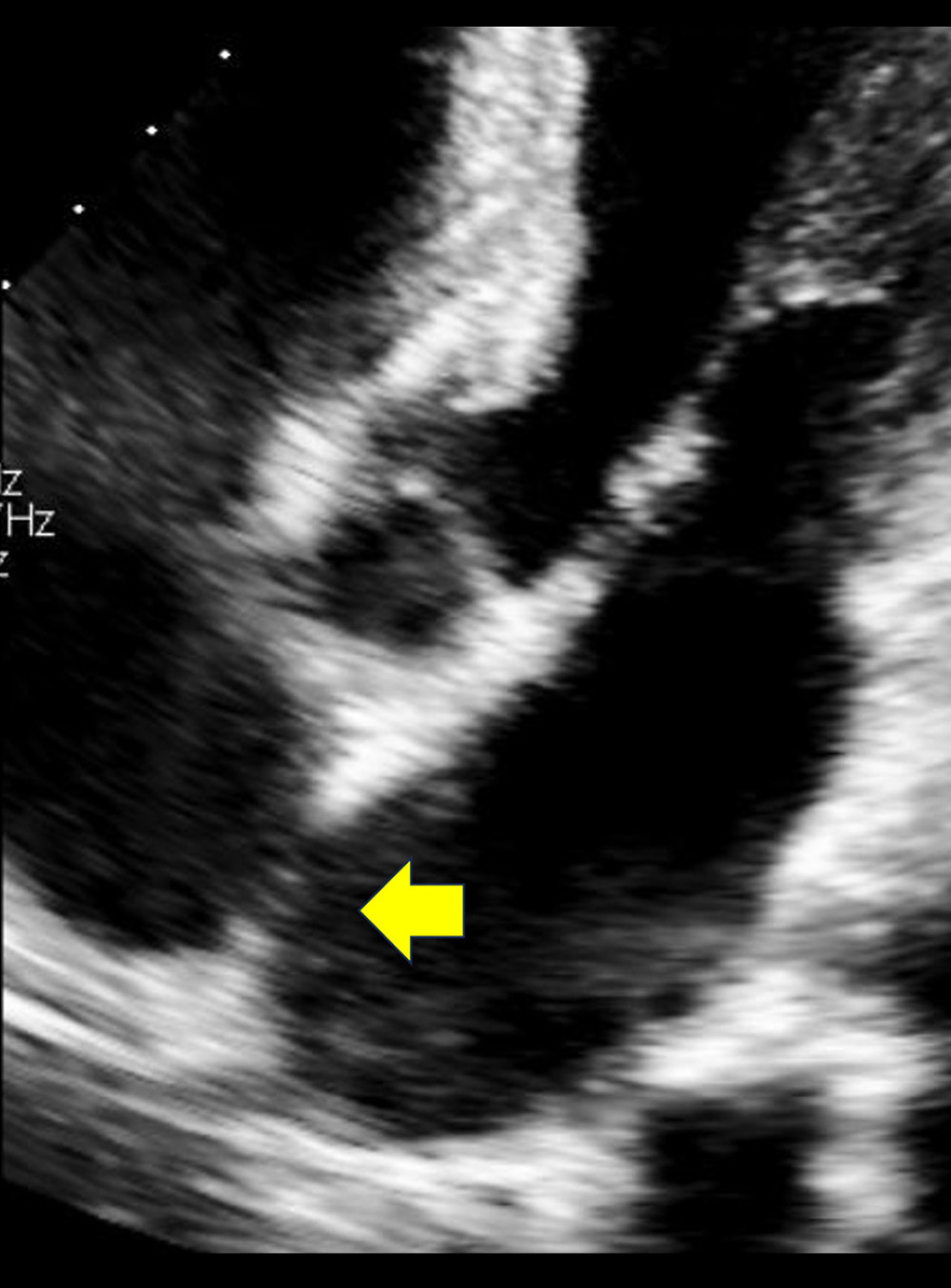 Figure 6. Postoperative transthoracic echocardiography shows no residual shunt.
Figure 6. Postoperative transthoracic echocardiography shows no residual shunt. References
1. Kodaira M, Kawamura A, Okamoto K, Comparison of clinical outcomes after transcatheter vs. minimally invasive cardiac surgery closure for atrial septal defect: Circ J, 2017; 81; 543-51
2. Mylonas KS, Ziogas IA, Evangelious A, Minimally invasive surgery vs device closure for atrial septal defects: A systematic review and meta-analysis: Pediatr Cardiol, 2020; 41; 853-61
3. Jung JC, Kim KH, Minimally invasive cardiac surgery versus conventional median sternotomy for atrial septal defect closure: Korean J Thorac Cardiovasc Surg, 2016; 49; 421-26
4. Baumgartner H, Bonhoeffer P, De Groot NM, ESC Guidelines for the management of grown-up congenital heart disease (new version 2010): Eur Heart J, 2010; 31; 2915-57
5. Kim K, Kim YS, Kim HR, Robotic repair of atrial septal defect: Pre-groove vertical right atriotomy approach: JTCVS Tech, 2024; 28; 73-81
Figures
Figure 1. Preoperative transthoracic echocardiography shows an atrial septal defect (yellow arrow).Figure 2. Preoperative transesophageal echocardiography shows a relatively small aortic rim of only 1 mm (yellow arrow).Figure 3. Preoperative computed tomography scan shows an atrial septal defect (yellow arrow).Figure 4. Preoperative computed tomography scan (volume rendering) shows an atrial septal defect (yellow arrow).Figure 5. Atrial septal defect patch closure was performed via the left atrial side approach using totally endoscopic minimally invasive cardiac surgery. The yellow arrow indicates the atrial septal defect margin; the green arrow represents the fabric sheet.Figure 6. Postoperative transthoracic echocardiography shows no residual shunt.In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133