09 April 2021: Articles 
Left Atrial Appendage Ostial Stenosis: A Case Report and Literature Review
Rare disease
Yuka Sakatani1BDEF*, Takahide Ito1ADF, Hitomi Hasegawa1D, Kanako Akamatsu1AB, Masaaki Hoshiga1ADOI: 10.12659/AJCR.930510
Am J Case Rep 2021; 22:e930510






Abstract
BACKGROUND: Left atrial appendage (LAA) ostial stenosis is a rare cardiac condition usually identified by transesophageal echocardiography (TEE). LAA ostial stenosis can be classified into 2 types: one is idiopathic and the other is a complication after incomplete surgical LAA ligation. The former one is even rarer and only 12 cases have previously been reported.
CASE REPORT: An asymptomatic young woman was found at a medical checkup to have an abnormal jet signal in the left atrium on transthoracic echocardiography. TEE revealed that the abnormal signal originated from a narrowed orifice of the LAA. There were no other cardiac abnormalities in this woman. Unlike the previously reported cases, our case had LAA ostial stenosis detected by transthoracic echocardiography but not by TEE.
CONCLUSIONS: We describe a case of anatomic narrowing of the LAA orifice in a young woman. This was a first-ever case of idiopathic LAA ostial stenosis that was detected by transthoracic echocardiography. Because of the very small number of such cases reported, it remains unknown whether anticoagulation is required to prevent intra-atrial thrombus formation.
Keywords: Atrial Fibrillation, Atrial Function, Left, Echocardiography, Transesophageal, Atrial Appendage, Constriction, Pathologic
Background
Left atrial appendage (LAA) ostial stenosis is a rare cardiac condition mostly identified by transesophageal echocardiography (TEE). LAA ostial stenosis can be classified into 2 types: one is idiopathic with unknown etiologies, and the other is a complication occurring as a result of incomplete surgical ligation of the LAA. The former one is even rarer and only 12 cases have previously been reported. In all the cases, LAA ostial stenosis was discovered incidentally, and approximately half of them were complicated by atrial arrhythmia. We herein describe the former type of LAA ostial stenosis in a young woman in whom transthoracic echocardiography, but not TEE, was the first imaging tool leading to the diagnosis. We also provide a short review of clinical features in this particular condition.
Case Report
A 30-year-old woman was referred to our hospital for further examination of the heart, having been found to have an abnormal jet signal in the left atrium (LA) on transthoracic echo-cardiography. The echocardiography was performed because she had an abnormal electrocardiogram finding detected at the medical checkup. She had been treated for hypothyroidism for years, without a history of cardiac surgery.
Her height was 160 cm and her weight was 53 kg. The blood pressure was 116/78 mmHg. The physical examination was not remarkable; no heart murmur was audible. The electrocardiogram showed normal sinus rhythm with minor ST-T abnormalities. The chest X-ray showed normal cardiac silhouette, around which no noticeable shadows were present. On transthoracic echocardiography, there were normal chamber size and function (left ventricular diastolic dimension 44 mm; ejection fraction 65%; and left atrial diameter 33 mm) and no pathological changes in the heart valves. With color-flow mapping, a jet signal, running from the lateral to the medial, could be seen within the LA (Figure 1).
TEE performed for more detailed examination showed an abnormal jet signal within the LA which, occurring with atrial systole, appeared to originate from around the LAA orifice (Figure 2A). When the continuous, but not pulsed, Doppler sample volume was set around there, a high-velocity wave of the peak velocity >2.0 m/s was recorded (Figure 2B). On 2D examination, there was a membrane-like structure covering and narrowing the LAA orifice to a diameter of 3.0 mm (Figure 2C). A small LAA was located below the membrane-like structure, and found to be contracting vigorously. No intra-LAA thrombus was found. On real-time 3D imaging, a small LAA orifice could be seen (Figure 2D). Taking those findings and similar previously reported cases into consideration, such an LAA was diagnosed as LAA ostial stenosis.
Discussion
A report of 500 autopsy cases showed that the LAA orifice diameter in adult individuals measured 5 to 20 mm in men and 5 to 18 mm in women [1]. Among patients in sinus rhythm who had normal cardiac function, in addition, the peak LAA emptying velocity was 60±14 (standard deviation) cm/s [2]. In the current case, the LAA orifice diameter was calculated as 3.0 mm and the LAA emptying velocity as >2.0 m/s, indicating that our patient had a significant narrowing of the LAA orifice.
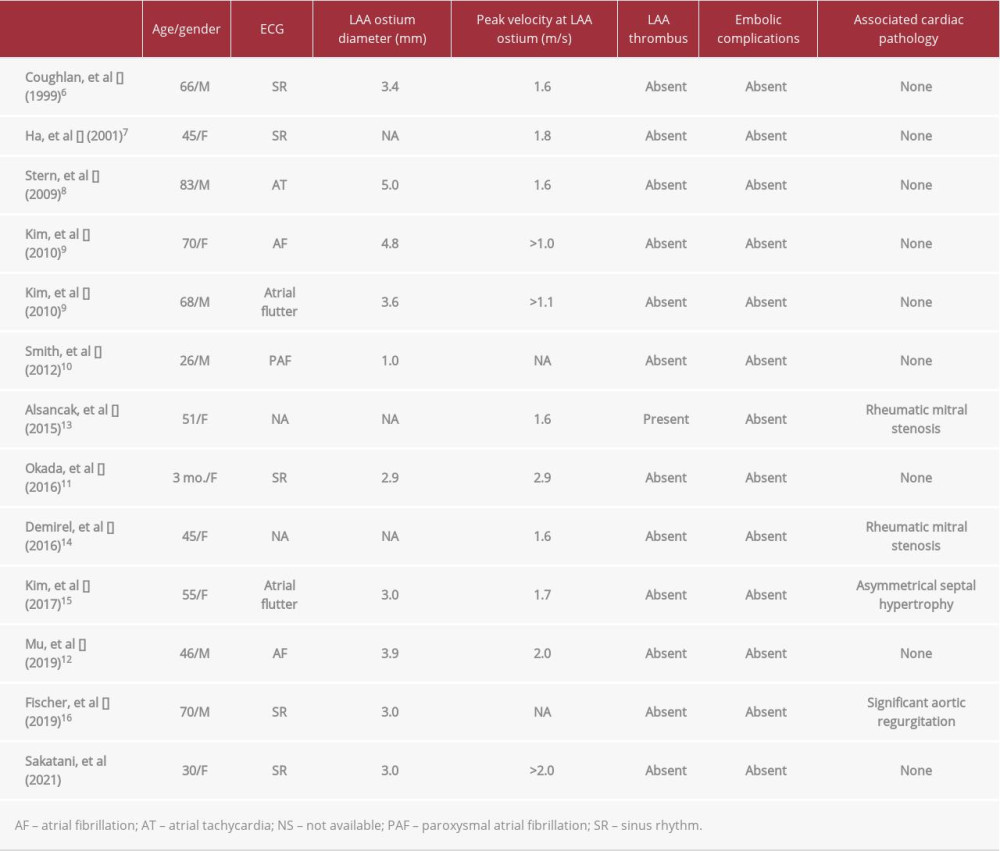
LAA ostial stenosis can be seen among patients whose LAA was ligated incompletely during cardiac surgery [3–5]. On the other hand, an idiopathic type of LAA ostial stenosis is even rarer. To the best of our knowledge, in the literature, a total of 12 cases of congenital LAA ostial stenosis were reported, 8 considered to be idiopathic [6–12] and the remaining 4 accompanied by pathological findings such as rheumatic mitral stenosis [13–16] (Table 1). The first case was described by Coughlan et al in 1999, in which a 66-year-old woman presenting with neurological symptoms was incidentally found to have LAA ostial stenosis during TEE [7].
The cause and clinical significance of an idiopathic type of LAA ostial stenosis remain unclear. Because of the membrane-like structure, some authors considered LAA ostial stenosis to be a variant of cor triatriatum, which has a congenital intra-atrial membranous structure that divides the main LA into the superior and inferior portions [6]. However, this is argued by the fact that the developmental origin is different between the LAA and the main LA; the former is the residual tissue of the embryonic LA that develops within 4 weeks of the fetal life, whereas the latter is formed later through the absorption of the primordial pulmonary veins [10,17–19]. In a pediatric case, whose sibling had cor triatriatum, it was suggested that they had an embryogenesis in common leading to a membranous structure [11]. Moreover, there were a few reports that LAA ostial stenosis was associated with rheumatic mitral disease, the authors of which suggested that some inflammatory process involved with rheumatic fever might be related to the developmental mechanism for a membrane-like structure [13,14].
Therapeutic implications of LAA ostial stenosis may also be uncertain. One surgical case suggested that LAA thrombus formation presumably resulting from incomplete LAA ligation might cause embolic complications [5]. On the other hand, neither LAA thrombus nor embolic events has been reported in idiopathic cases (Table 1). Even if LAA thrombus were formed, the narrowed orifice opened to the main LA would hamper it from moving into the systemic circulation.
Unlike the previously reported cases, our case had LAA ostial stenosis detected in the wake of transthoracic echocardiography, but not TEE. With the patient’s age, cardiac condition, and unlikeliness of intracardiac thrombus formation for idiopathic cases taken into consideration, the patient had not received any cardiac medications, including anticoagulation.
Nevertheless, follow-up at least every few years was considered necessary to monitor for pathological alterations related to thrombus formation, including atrial arrhythmia. To the best of our knowledge, our case is the second one in which the narrowed LAA ostium was imaged by 3D TEE [12]. Other imaging modalities such as computed tomography and magnetic resonance imaging could have more convincingly confirmed this rare entity [10,13,16].
Conclusions
We describe a case of anatomic narrowing of the LAA orifice of unknown etiologies in a young woman. This was a first-ever case of LAA ostial stenosis that was detected in the wake of transthoracic echocardiography. With a very small number of such cases reported, it remains unknown whether anticoagulation should be directed to prevent intra-atrial thrombus formation.
Figures
References:
1.. Venoit JP, Harrity PJ, Gentile F, Anatomy of the normal left atrial appendage. A quantitative study of age-related changes in 500 autopsy hearts: Implications for echocardiographic examination: Circulation, 1997; 96; 3112-15
2.. Tabata T, Oki T, Fukuda N, Influence of aging on left atrial appendage flow velocity patterns in normal subjects: J Am Soc Echocardiogr, 1996; 9; 274-80
3.. Katz ES, Tsiamtsiouris T, Applebaum RM, Surgical left atrial appendage ligation is frequently incomplete: a transesophageal echocardiographic study: J Am Coll Cardiol, 2000; 36; 468-71
4.. Lynch M, Shanewise JS, Chang GL, Recanalization of the left atrial appendage demonstrated by transesophageal echocardiography: Ann Thorac Surg, 1997; 63; 1774-75
5.. Fisher DC, Tunick PA, Kronzon I, Large gradient across a partially ligated left atrial appendage: J Am Soc Echocardiogr, 1998; 11; 1163-65
6.. Coughlan B, Lang RM, Spencer KT, Left atrial appendage stenosis: J Am Soc Echocardiogr, 1999; 12; 882-83
7.. Ha JW, Chung N, Hong YS, Left atrial appendage stenosis: Echocardiography, 2001; 18; 295-97
8.. Stern JD, Skolnick AH, Freedberg RS, Isolated left atrial appendage ostial stenosis: Eur J Echocardiogr, 2009; 10; 702-3
9.. Kim S, Shim WJ, Park SM, Two cases of incidentally diagnosed idiopathic left atrial appendage ostial stenosis: J Cardiovasc Ultrasound, 2010; 18; 112-14
10.. Smith C, Hunt M, Geimer-Flanders J, An incidentally discovered left atrial appendage membrane: case report and leterature review: Hawaii J Med Public Health, 2012; 71; 103-5
11.. Okada S, Ishiguchi Y, Moritoh Y, Siblings with idiopathic left atrial appendage ostial stenosis and cor triatriatum: Echocardiography, 2016; 33; 1098-100
12.. Mu L, Li M, Wang Y, Idiopathic left atrial appendage ostial stenosis detected by 3D transoesophageal echocardiography: Eur Heart J Cardiovasc Imaging, 2019; 20; 722
13.. Alsancak Y, Sezenoz B, Öncü F, Left atrial appendage ostial stenosis associated with rheumatic mitral stenosis: Anatol J Cardiol, 2015; 15; E11-12
14.. Demirel M, Toprak C, Acar E, Left atrial appendage ostial stenosis in a patient with rheumatic mitral valve desease: Turk Kardiyol Dern Ars, 2016; 44; 533
15.. Woohyeun K, Won YJ, Eun JP, Left atrial appendage ostial stenosis in a patient with atrial flutter and asymmetric septal hypertrophy: J Cardiol and Cardiovasc Ther, 2017; 7; 555721
16.. Jonas F, Cornelia J, Niemann T, Left atrial appendage stenosis: Cardiovasc Med, 2019; 22; w02029
17.. Beigel R, Wunderlich NC, Ho SY, The left atrial appendage: Anatomy, function, and noninvasive evaluation: JACC Cardiovasc Imaging, 2014; 7; 1251-65
18.. Patti G, Pengo V, Marcucci R, From embryology to prevention of thromboembolism: Eur Heart J, 2017; 38; 877-87
19.. Al-Saady NM, Obel OA, Camm AJ, Left atrial appendage: structure, unction, and role in thromboembolism: Heart, 1999; 82; 547-54
Figures
In Press
14 Mar 2024 : Case report ")
Am J Case Rep In Press; DOI: 10.12659/AJCR.942826
14 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.942770
16 Mar 2024 : Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.943214
16 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943010
Most Viewed Current Articles
07 Mar 2024 : Case report 
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250