11 November 2021: Articles 
Sedation and Acute Encephalopathy in a Pediatric Patient Following Ingestion of Delta-8-Tetrahydrocannabinol Gummies
Unusual clinical course, Management of emergency care, Clinical situation which can not be reproduced for ethical reasons
Peter Akpunonu1ABCDEF*, Regan A. Baum2ABCDEF, Andrew Reckers3ABCDEF, Blake Davidson4ABCDEF, Ross Ellison3ABCDEF, Matthew Riley4ABCDEF, Jordan Trecki5ABCDEF, Roy Gerona3ABCDEFDOI: 10.12659/AJCR.933488
Am J Case Rep 2021; 22:e933488






Abstract
BACKGROUND: Delta-8 tetrahydrocannabinol (delta-8 THC) is an isomer of delta-9-tetrahydrocannabinol (delta-9 THC), the primary psychoactive cannabinoid in the marijuana plant. Typically found at lower concentrations in marijuana, delta-8 THC exhibits psychoactive properties similar to delta-9 THC. Products containing delta-8 THC are readily available across the US and currently there is a lack of available confirmatory testing specific to delta-8 THC as there is cross-reactivity to other naturally occurring cannabinoids in standard immunoassays. Pediatric exposures to this substance are on the rise.
CASE REPORT: We present a case with laboratory confirmation of a previously healthy 2-year-old girl ingesting approximately 15 mg/kg of delta-8 THC gummies. The patient arrived minimally responsive and requiring intubation for encephalopathy. Laboratory confirmation of delta-8 THC exposure is not routinely available with common testing modalities. A urine drug screen preformed in the hospital was positive for delta-9 THC. With the collaboration of the Drug Enforcement Administration’s Toxicology Testing Program, detection and confirmation of delta-8 THC was performed in the serum and urine using liquid chromatography-quadrupole time-of-flight mass spectrometry.
CONCLUSIONS: The prevalence of delta-8 THC-containing products in the illicit drug market is increasing rapidly. Delta-8 THC products are now available in gas stations and in headshops. The clinical presentation of delta-8 THC exposure is similar to known effects of delta-9 THC exposure. These similarities limit the clinicians’ abilities to determine the specific substance ingested. Symptomatic and supportive care remains an effective treatment for cannabinoid toxicity.
Keywords: Cannabidiol, illicit drugs, Intensive Care Units, Pediatric, marijuana use, Brain Diseases, Cannabinoids, Child, Child, Preschool, Dronabinol, Eating, Female, Humans
Background
Delta-8-tetrahydrocannabinol (delta-8 THC) is an isomer of delta-9-tetrahydrocannabinol (delta-9 THC). While both substances are found in the marijuana plant, delta-8 THC is typically found in much lower concentrations than delta-9 THC [1,2]. Delta-9 THC, the primary psychoactive cannabinoid in marijuana, is responsible for a range of symptoms observed following exposure in children, including simple difficulty ambulating, excessive sleepiness, respiratory depression, or seizures [3,4]. Less commonly, children have developed coma and required intubation and the use of a ventilator [4]. The increased availability of THC-containing products, especially those appealing to children such as gummies, candies, or cookies, have resulted in an increase in accidental exposure to younger individuals. The recent increase in marketing of delta-8 THC-containing edibles and vaping products has resulted in both adult and pediatric exposure resulting in adverse effects, including children requiring intensive care unit (ICU) admissions following exposure [5].
Case Report
Our patient was a previously healthy 2-year-old girl who was transferred via air ambulance for sedation and decreased responsiveness following a reported “CBD edibles” ingestion. Ingestion was determined to be approximately 45 minutes prior to arrival at the local hospital. On arrival to the local emergency department (ED), the child was minimally responsive to stimuli, with a Glasgow Coma Scale of three. The patient weighed 15.3 kg. Vitals were a heart rate of 136 beats per minute, with an O2 saturation of 98% on room air. Given her acute encephalopathy, there was concern for airway compromise and she was intubated using fentanyl and ketamine.
On arrival to the ED, she remained minimally responsive but did have spontaneous eye opening and upper-extremity movements. The patient was placed on dexmedetomidine drip at 0.5 mcg/kg/h for light sedation and admitted to the pediatric intensive care unit.
The toxicology service was consulted and presented to bedside to evaluate the patient. The father stated he had purchased delta-8 THC gummies from a local gas station, leaving the unopened product on a desk. Later, the family noted the patient was behaving oddly and was lethargic. The family investigated and found an open empty package of gummies with three spilled on the floor. The package contained 12 gummies, each containing 25 mg of delta-8 THC according to the manufacture’s labeling. The father estimated the ingestion to be approximately nine gummies, yielding an estimated total dose of 225 mg of delta-8 THC (14.7 mg/kg). The father denied access to other marijuana products in the home.
An initial urine drug screen (UDS) was performed via enzyme-linked immunoassay (ELISA), which was positive for cannabinoids and fentanyl. Reflex liquid chromatography-tandem mass spectrometry (LC-MS/MS) detected fentanyl at 5 ng/ml and carboxy-THC at >400 ng/ml. Comprehensive urine drug testing by gas chromatography-mass spectrometry (GC-MS) revealed ketamine, fentanyl, and cannabinoids. Her complete blood count and comprehensive metabolic panel did not reveal any significant abnormalities.
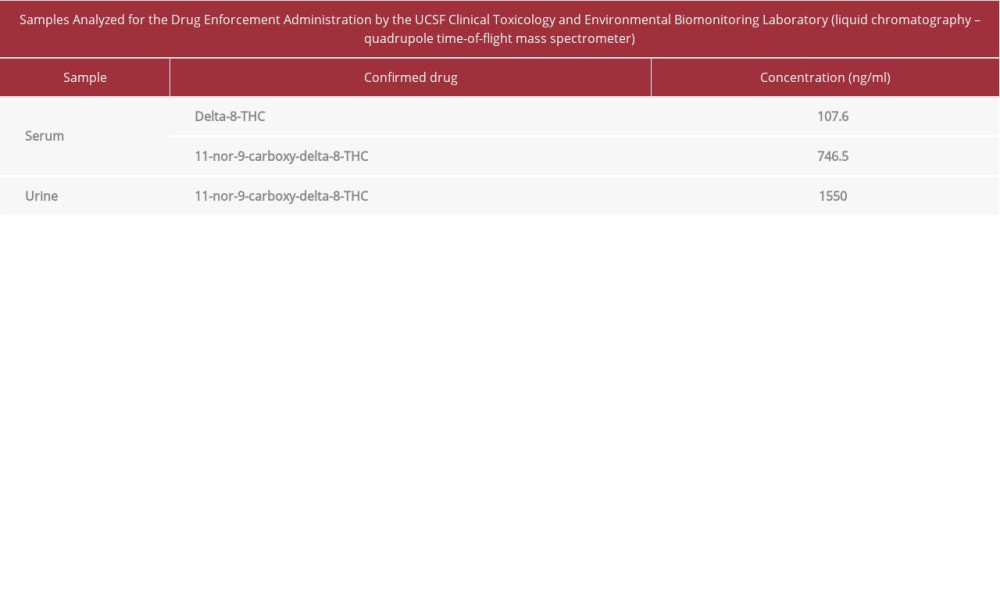
The child’s biological samples and the gummies were referred to the Drug Enforcement Administration’s Toxicology Testing Program (DEA TOX) for analysis. Comprehensive drug analysis using liquid chromatography-quadrupole time-of-flight mass spectrometry (LC-QTOF/MS) confirmed delta-8 THC and the absence of delta-9 THC in the gummy. The plasma concentration was 107.6 ng/mL delta-8 THC and 746.5 ng/mL 11-nor-9-carboxy-delta-8-THC, while the urine concentration was 1550 ng/mL 11-nor-9-carboxy-delta-8-THC. Results are summarized in Table 1.
The patient was extubated approximately 10 hours after arrival at the pediatric intensive care unit (PICU) and monitored on the pediatric floor for an additional 24 hours. Her mental status changes resolved, GCS returned to 15, and she was able to tolerate oral foods and liquids. Her mental impairment resolved after an additional 24 hours and, following recommendations by social work and pediatric forensics, she was discharged home.
Discussion
CURRENT EVIDENCE:
Research into the cannabinoid pharmacology was driven by the discovery and isolation of the two most common cannabinoids, delta-9 THC and cannabidiol. Since their discovery in the 1930s and 1940s, many other cannabinoids have been identified. Cannabinoid concentrations vary greatly between plants and, although not a recent discovery, delta-8 THC has more recently gained popularity, with articles published in mainstream media. Initial investigations into delta-8 THC began in the 1970s with investigation of antineoplastic and antiemetic properties in animal models [6–8]. Delta-8 THC occurs in trace amounts in the cannabis plant and could be a degradation product of delta-9 THC after long-term storage and aging [2].
PHARMACOLOGY:
Pharmacologically, delta-8 THC, like delta-9 THC, has agonistic properties at both the cannabinoid type 1 and type 2 receptors [8–10]. Relatively few studies have evaluated the potency of delta-8 THC compared to delta-9 THC. A study in mice suggested near-equivalent potency of delta-8 THC vs delta-9 THC [6]. One of the mouse studies characterized three progressive stages of exposure to both delta-9 THC and delta-8 THC: (1) irritability; (2) decrease in spontaneous activity, with hyper-sensitivity to auditory and tactile stimuli; and (3) marked depression of spontaneous activity, decreased awareness, loss of muscle coordination, and reduced sensorimotor response [6]. A higher incidence of “freezing” or immobility in delta-8 THC exposures was also documented. Additionally, hypothermia and respiratory depression were noted with both compounds [6].
CLINICAL PRESENTATION:
It has previously been reported that the psychoactive effects of delta-8 THC are qualitatively similar to delta-9 THC in children and adults [8,12]. In a small open-label study, delta-8 THC administered as an antiemetic in pediatric oncology patients abated vomiting in all eight individuals who received treatment. Adverse effects included irritability (two subjects) and euphoria (one subject) [8]. In a study of adult volunteers, delta-8 THC administered either orally or intravenously was reported to be slightly less potent than delta-9 THC, with an estimated potency ratio of 2: 3. In this study, six male subjects were administered oral doses of either 20 mg of delta-8 THC, an equal dose of delta-9 THC, or a 40-mg dose of delta-8 THC contained in chocolate cookies. The authors stated all three doses produced similar somatic, perceptual, and psychic effects. Somatic effects appeared early and included dizziness, dryness of mucous membranes, paresthesia, tinnitus, increased body awareness, weakness, muscle tension or tremor, incoordination, fatigue, and sleepiness. Perceptual effects appeared concurrently with psychic effects, and, although not as prominent, included blurring, vibrations, or distortions of vision, such as altered perspectives, imagery, and enhancement of colors or contrasts; time distortion, and decreased discrimination of hearing. Psychic effects included euphoria, tranquility, and relaxation; difficulty in thinking, speaking, reading, remembering; unusually rapid flow of thoughts; and dreamy, introspective states [12]. Following intravenous administration of delta-8 THC to three males, the qualitative symptoms experienced were similar to those reported from delta-9 THC. While subjects within the study reported that delta-8 THC had slightly weaker effects as compared to delta-9 THC [12], the study conducted a subjectively rated dose-response curve to compare effects of both substances, with no significant differences in dose-effect curves for these two substances.
A wide variety of symptoms can develop from profound delta-9 THC exposure in children, from simple difficulty ambulating, to excessive sleepiness, to respiratory depression [13]. Coma requiring mechanical ventilation has been rarely reported in exposed children. Symptoms can range from being unbalanced, to any degree of sleepiness, to poor respiratory effort. Less commonly, children have developed coma and required intubation [13].
MANAGEMENT:
Symptomatic and supportive care remains an effective treatment for cannabinoid toxicity. Gastrointestinal decontamination is generally not recommended for oral ingestions due to the decline in mental status or acute agitation. Intravenous fluids and vasopressors can be considered for hemodynamic support, and benzodiazepines can be administered for anxiety, agitation, or seizures. The collection of drug samples in addition to patient blood and urine may aid in further understanding effects and treatment requirements [14].
TESTING:
There are no published case reports of delta-8 THC exposures to date nor has there been laboratory confirmation obtained. The lack of available confirmatory testing specific to delta-8 THC and its cross-reactivity to other naturally occurring cannabinoids in standard immunoassays, along with similarities in presentation to delta-9 THC exposures, present a challenge to properly documenting delta-8 THC intoxications [2]. Recently, an LC-MS/MS method to confirm delta-8 THC and its metabolites in Driving Under the Influence of Drugs investigation casework was published [15]. However, no method using LC-QTOF/MS, as applied in our case, has previously been published.
PRODUCTS:
Products containing delta-8 THC are readily available across the US via online sources, in gas stations, and in headshops. Delta-8 THC-containing products come labeled as having metabolites with the potential to trigger drug tests for delta-9 THC and should be avoided if a drug test is imminent. Large quantities of delta-8 THC can be purchased as edibles, various infused plant products, via atomizer devices, tinctures, and as bulk product. As with delta-9 THC, concentration and labeling varies greatly depending on the sources and manufacturer.
Conclusions
As the availability of delta-8 THC increases, we can anticipate exposures to these products will increase. Currently, it is difficult to differentiate delta-8 THC from delta-9 THC utilizing routine laboratory testing. The clinical presentation of delta-8 THC exposure is consistent with the known effects of delta-9 THC, limiting clinician abilities to determine the specific substance ingested. Current commercially available packaging and flavoring do little to deter children from ingesting these substances.
References:
1.. ElSohly MA, Chandra S, Radwan M, A comprehensive review of cannabis potency in the United States in the last decade: Biol Psychiatry Cogn Neurosci Neuroimaging, 2021; 6(6); 603-6
2.. , Cannabis: From cultivar to chemovar II – a metabolomics approach to cannabis classification, 2016; 1(1); 202-215
3.. Emoto J, Weeks K, Kallail KJ, Accidental acute cannabis intoxication presenting as seizure in pediatrics patients: Kans J Med, 2020; 13; 129-30
4.. Wang GS, Pediatric concerns due to expanded cannabis use: Unintended consequences of legalization: J Med Toxicol, 2017; 13(1); 99-105
5.. , Health advisory: Increases in availability of cannabis products containing delta-8 THC reported cases of adverse events September 14; 2021 https://www.emergency.cdc.gov/han/2021/han00451.asp
6.. Christensen HD, Freudenthal RI, Gidley JT, Activity of delta8- and delta9-tetrahydrocannabinol and related compounds in the mouse: Science, 1971; 172(3979); 165-67
7.. Dwivedi C, Harbison RD, Anticonvulsant activities of delta-8 and delta-9 tetrahydrocannabinol and uridine: Toxicol Appl Pharmacol, 1975; 31(3); 452-58
8.. Abrahamov A, Abrahamov A, Mechoulam R, An efficient new cannabinoid antiemetic in pediatric oncology: Life Sci, 1995; 56(23–24); 2097-102
9.. Bow EW, Rimoldi JM, The structure-function relationships of classical cannabinoids: CB1/CB2 modulation: Perspect Medicin Chem, 2016; 8; 17-39
10.. Pertwee RG, The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin: Br J Pharmacol, 2008; 153(2); 199-215
11.. Grotenhermen F, Pharmacokinetics and pharmacodynamics of cannabinoids: Clin Pharmacokinet, 2003; 42(4); 327-60
12.. Hollister LE, Gillespie HK, Delta-8- and delta-9-tetrahydrocannabinol comparison in man by oral and intravenous administration: Clin Pharmacol Ther, 1973; 14(3); 353-57
13.. Macnab A, Anderson E, Susak L, Ingestion of cannabis: A cause of coma in children: Pediatr Emerg Care, 1989; 5(4); 238-39
14.. Lapoint JM, Cannabinoids: Goldfrank’s Toxicologic Emergencies, 2019, New York, NY, McGraw-Hill Education
15.. Chan-Hosokawa A, Nguyen L, Lattanzio N, Adams WR, Emergence of delta-8 tetrahydrocannabinol (THC) in DUID Investigation casework: Method development, validation and application: J Anal Toxicol, 2021 [Online ahead of print]
In Press
05 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.942032
06 Mar 2024 : Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.942937
12 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943244
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943275
Most Viewed Current Articles
07 Mar 2024 : Case report
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250