29 November 2022: Articles 
Diagnostic Pitfalls of Chylothorax After Dasatinib Treatment of Chronic Myeloid Leukemia
Unknown etiology, Mistake in diagnosis, Adverse events of drug therapy
Ryan L. Kelly1EF*, Ju Young BaeDOI: 10.12659/AJCR.938319
Am J Case Rep 2022; 23:e938319






Abstract
BACKGROUND: Chronic myeloid leukemia (CML) is a myeloproliferative malignancy generally treated with Dasatinib, a tyrosin-kinase inhibitor. Pleural effusions are a known adverse effect, but only 0.8% of patients develop pleural effusions after 6 years of use. Recent case reports have implicated Dasatinib as a rare cause of chylothorax.
CASE REPORT: We describe a woman in her 30’s with a history of chronic myeloid leukemia, who had been taking Dasatinib for 10 years and presented to the Emergency Department after a chest X-ray revealed bilateral pleural effusions in the setting of worsening dyspnea on exertion for 6 months. She had previously received radiotherapy at age 11 prior to an allogenic bone marrow transplant nearly 30 years prior. Thoracentesis removed 900 cc of chylous fluid, and flow cytometry and cultures found no evidence of infection or malignancy. Dasatinib was discontinued, and she was treated with diuretics, steroids, and a low-fat diet. The effusions reaccumulated twice in the following month and required 2 additional thoracenteses and courses of steroids. Months later, the bilateral chylous effusions recurred, and MR lymphangiogram demonstrated 2 thoracic duct tears.
CONCLUSIONS: While previous reports have indicated that Dasatinib can rarely cause chylous pleural effusions, it is unlikely after 5 years of use, and other etiologies must be considered by clinicians. Initial misattribution to Dasatinib alone can delay further necessary investigations, including lymphangiography. In our patient, it is more likely that other factors contributed to her chylothorax, including her previous radiotherapy 30 years prior, given her recurrence of chylous effusions following cessation of the medication.
Keywords: chylothorax, dasatinib, Female, Humans, Child, Leukemia, Myelogenous, Chronic, BCR-ABL Positive, Thoracic Duct, Pleural Effusion
Background
Chronic myeloid leukemia (CML) is a myeloproliferative malignancy generally traced to a single genetic abnormality of the Philadelphia chromosome, a result of the t(9,22) forming a BCR-ABL 1 fusion gene [1]. As a consequence of this mutation, this gene is a constitutively active tyrosine kinase, promoting uncontrolled cell growth as an oncoprotein. Dasatinib, a tyrosine kinase inhibitor, is a first-line therapy for the medical management in CML. Commonly, Dasatinib use is associated with pleural effusions, with 1 study noting 26% of CML patients developing effusions while on this medication [2]. Recent case reports have implicated Dasatinib as a rare cause of chylothorax [3–12]. One study that patients on Dasatinib followed for 7 years calculated 60.1 weeks as the median onset for the development of pleural effusions, and only 0.8% of patients developed a pleural effusion after 6 years [13]. In this paper, we present the case of a woman in her 30’s who was diagnosed with a medication-induced chylothorax following a 10-year history of Dasatinib use, yet after repeated recurrences of pleural effusions, she was later found to have 2 thoracic duct tears. This case report details the extensive diagnostic workup that should be considered to investigate other potential causes of chylothorax, given the rarity of Dasatinib causing this adverse effect after 10 years of use.
Case Report
INITIAL PATIENT PRESENTATION:
A woman in her 30’s originally presented to a pulmonologist with a concern of dyspnea for 6 months. She noted acute worsening of symptoms after receiving her first COVID-19 vaccine. A chest X-ray revealed new bilateral pleural effusions. The patient’s oncology history was significant for a diagnosis of chronic myeloid leukemia (CML) at age 11, which was treated with total body irradiation and an allogeneic bone marrow transplant. The CML recurred at age 29, and the patient was treated with a repeat bone marrow transplant and started on Dasatinib 50 mg daily. The patient had not reported any known adverse effects during the past 10 years while taking this medication. Other past medical history was significant for premature ovarian failure (on Norethindrone-ethinyl estradiol) and hypothyroidism. She denied any history of smoking or tobacco use.
PHYSICAL EXAM FINDINGS:
On presentation in the Emergency Department, her vital signs were temperature 36.6°C, heart rate of 91 beats per minute, respiratory rate of 18 breaths per minute, blood pressure 168/100 mmHg, and oxygen saturation of 95% on room air. A physical exam demonstrated decreased breath sounds in the middle and lower lung fields bilaterally with dullness to percussion at the bases. Her lungs were clear in the upper lung fields. Thyromegaly was present and the rest of the physical exam was unremarkable.
INVESTIGATION FINDINGS:
Laboratory test results on admission are outlined in Table 1 and were significant for abnormal inflammatory markers (CRP, ESR), D-dimer, and lipid panel. SARS-CoV-2 PCR testing via nasal swab was negative. Electrocardiography demonstrated normal sinus rhythm. Computed tomography angiography (CTA) of her chest revealed no evidence of pulmonary embolism but did find large bilateral pleural effusions and right upper-lobe alveolar infiltrates (Figure 1). Transthoracic echocardiography showed normal biventricular size and systolic function, no significant valve abnormalities, and a small anterior pericardial effusion without significant hemodynamic effect. The patient subsequently underwent a left thoracentesis, with 900 cc of chylous pleural fluid collected. Results of the pleural fluid analysis are outlined in Table 1, and were consistent with an exudative effusion. Acid-fast bacteria, fungal, and body fluid cultures were negative for growth after a 6-week period. The pleural fluid was 77% lymphocyte-predominant. Flow cytometry showed a normal immunophenotype with mixed lymphocytes and no evidence for monoclonal non-Hodgkin B-cell lymphoproliferative disease. Cytology of the pleural fluid was negative for evidence of malignancy.
DIFFERENTIAL DIAGNOSIS:
During the patient’s initial presentation, the likelihood of Dasatinib contributing to the pleural effusions was considered unlikely given the patient had taken the medication for 10 years without problems. However, the alternative explanations were considered even less plausible. Based on the data available, traumatic causes were considered unlikely given that she had never had surgery of the thorax or the lower neck nor had she previously undergone central line placement or pacemaker implantation. She also denied any history of blunt trauma to the chest. However, lymphangiogram and thoracic duct embolization were considered but were deferred by patient due to resolution of symptoms. Among non-traumatic causes, malignancy was considered the most likely potential etiology, but there were no imaging, flow cytometry, or cytology results that would suggest a malignancy. Infectious etiologies of chylothorax were considered even more unlikely given her clinical presentation with no apparent signs/symptoms of infections such as tuberculosis or histoplasmosis. Congestive heart failure is not a known cause of chylothorax, and the TTE found no evidence of causes of heart failure. With Dasatinib being a known cause of chylous pleural effusions, the clinical team attributed the pleural effusions to the medication.
TREATMENT AND OUTCOME:
Dasatinib was held, and she was started on corticosteroids and diuretics, with improvement. However, her pleural effusions recurred, and she required 2 additional thoracenteses and courses of prednisone, removing 900 mL and 725 mL of chylous fluid, respectively. Following these procedures, she was considered for a lymphatic angiogram, but this was deferred due to her sustained clinical improvement, and she opted to adhere to a strict low-fat diet. With the resolution of our patient’s symptoms off of Dasatinib, the medication was not resumed.
The patient continued to remain in remission and without further accumulation of pleural effusions while being monitored off Dasatinib for 6 months until she had a recurrence of bilateral chylothorax. Repeat thoracentesis removed 500 cc of chylous fluid. Four months later, the patient was referred for an MR lymphangiogram, which identified 2 tears in the thoracic duct. At this time, the etiology of the patient’s chylothorax was no longer thought to be due to her Dasatinib usage. She subsequently underwent a thoracic duct embolization and repeat left thoracentesis. The procedure was tolerated without any complications.
Discussion
Chylothorax is commonly attributed to a traumatic injury of the thoracic duct, including postoperative complications, causing leakage of chyle into the pleural cavity. Atraumatic causes, such as malignancy or infection, can occur through direct involvement of the thoracic duct, and bulky lymph nodes causing compression and invasion of the thoracic duct [14]. Previous case reports have described chronic lymphocytic leukemia (CLL) as a potential cause of chylothorax [15]. Outside of direct compression of the thoracic duct, it has been proposed that sludging from an expanded population of atypical lymphocytes may lead to thoracic duct expansion and increased susceptibility to rupture [16]. However, there have been no reports suggesting a connection between chronic myeloid leukemia and chylothorax independent of induction by medication. In many of these cases, treatment of a chylothorax only requires direct drainage of the effusion and medical management with success seen through a strict low-fat diet or even the use of somatostatin and octreotide [17]. For patients who do not respond to medical management, lymphatic embolization or lymphatic ligation via angiogram can be considered [17].
Drug interactions rarely cause the formation of chylous effusions, with few medications being associated with chylothoraxes. One recent case report has attributed the renal cell carcinoma chemotherapeutic, Pazopanib, to the formation of a chylothorax [18]. However, in most case repors, drug-induced chylous effusions have been associated with Dasatinib. While the mechanism of this is not fully known, a recent study utilizing a rat animal model found that Dasatinib increased the permeability of pulmonary endothelial cells and pulmonary lymphatics [19]. These vascular changes may occur through a Dasatinib-induced inhibition of platelet-derived growth receptor β and SRC-family kinases, which subsequently decrease interstitial fluid pressure and increase vascular permeability [13]. It is unclear why Dasatinib has such a high specificity for the vasculature and lymphatics of the lungs.
Several recent case reports have been published demonstrating the relationship between Dasatinib and chylothorax formation (Table 2). All of these patients had been on Dasatinib for 4 years or less prior to diagnosis of chylothorax, with most having failed a previous treatment including Imatinib. Our patient tolerated Dasatinib for 10 years prior to symptom onset, indicating that a Dasatinib adverse effect may have been less likely. Whether there are any risk factors that predispose a CML patient on Dasatinib to form a chylothorax is unknown at this time.
In review of previous case reports [3–12], treatment of Dasatinib-induced chylothorax required supportive treatment, including a thoracentesis, diuretics, and steroids. Definitive treatment pertained to the cessation of Dasatinib. Effusion recurrence has been seen in patients who attempted to restart the medication or reduce the dosage [5,9,11]. On-going chronic myeloid leukemia treatment can be continued by switching to a similar tyrosine kinase inhibitor, such as Nilotinib, Bosutinib, or Imatinib.
While our patient was originally diagnosed with a medication-induced chylothorax, the later recurrence of the chylous effusions, with newly discovered thoracic duct tears, complicated the diagnosis. Upon further investigation into the patient’s history, it was discovered that she had had whole-body radiation at age 11, which has been shown to cause chylothoraxes [20]. If solely caused by the radiation therapy, it is unclear why these complications would have developed nearly 30 years later. However, given the discovery of multiple thoracic duct tears and recurrence of symptoms following cessation of Dasatinib, it is unlikely that Dasatinib alone caused our patient’s presentation. Multiple factors may be involved, including the course of radiation, taking Dasatinib, the underlying chronic myeloid leukemia, and other unknown contributors. It is unlikely that the patient developed complications from Dasatinib after 10 years of use, and clinicians should be reluctant to attribute Dasatinib to use of chylothoraxes after 5 years. Chylous effusions secondary to Dasatinib use have been most commonly described in the first 12 months following drug initiation (Table 2). At this time, the patient remains off Dasatinib and will continue to be monitored following her embolization.
Conclusions
Chylothorax formation is a rare complication resulting from treatment with Dasatinib, a commonly used and highly effective medication for CML. Treatment for Dasatinib-induced chylous effusions includes diuretics, steroids, and a low-fat diet, as well as cessation of Dasatinib. Chylous effusions can occur in patients after a prolonged course of Dasatinib, but this is unlikely after 5 years of use, so a broad diagnostic workup should be considered before attributing chylous effusions to Dasatinib, including infectious workup, echocardiogram, lymphangiogram, flow cytometry, and cytology. Early misattribution to Dasatinib can delay further investigative measures, including lymphangiogram in our patient’s case, and prolong the implementation of definitive treatments.
References:
1.. Jabbour E, Kantarjian H, Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring: Am J Hematol, 2020; 95(6); 691-709
2.. Maiti A, Cortes JE, Patel KP, Long-term results of frontline dasatinib in chronic myeloid leukemia: Cancer, 2020; 126(7); 1502-11
3.. Huang YM, Wang CH, Huang JS, Dasatinib-related chylothorax: Turk J Haematol, 2015; 32(1); 68-72
4.. Sasaki H, Kimizuka Y, Ogata H, Successful control of dasatinib-related chylothorax by the Japanese herbal medicine “Goreisan”: Intern Med, 2019; 58(21); 3139-41
5.. Al-Abcha A, Iftikhar MH, Abu Rous F, Laird-Fick H, Chylothorax: Complication attributed to dasatinib use: BMJ Case Rep, 2019; 12(12); e231653
6.. Baloch ZQ, Abbas SA, Bhatti H, Braver Y, Ali SK, Dasatinib-induced chylothorax in chronic myeloid leukemia: Proc (Bayl Univ Med Cent), 2017; 30(1); 71-73
7.. Hickman K, Diaz E, Graham R, Dasatinib-induced chylothorax in chronic myelogenous leukemia in pediatric patient: Report of a case and review of literature: J Pediatr Hematol Oncol, 2020; 42(7); e665-67
8.. Hsu CC, Hsu JF, Wu KL, Dasatinib-induced chylothorax in a patient with chronic myeloid leukaemia: A case report and literature review: Respirol Case Rep, 2021; 9(6); e00753
9.. Ferreiro L, San-José E, Suárez-Antelo J, Valdés L, Dasatinib-induced pleural effusion: Chylothorax, an option to consider: Ann Thorac Med, 2016; 11(4); 289-93
10.. Yang L, Lu N, Jing Y, Yu L, [Chylothorax related with dasatinib in the treatment of chronic myeloid leukemia: Report of 3 cases.]: Zhongguo Shi Yan Xue Ye Xue Za Zhi, 2016; 24(5); 1348-53 [In Chinese]
11.. Chen B, Wu Z, Wang Q, Dasatinib-induced chylothorax: Report of a case and review of the literature: Invest New Drugs, 2020; 38(5); 1627-32
12.. Molina V, Vañes S, Castelló C, Chiner E, Chylothorax secondary to dasatinib: Arch Bronconeumol (Engl Ed), 2020; 56(9); 599-601
13.. Cortes JE, Jimenez CA, Mauro MJ, Geyer A, Pleural effusion in dasatinib-treated patients with chronic myeloid leukemia in chronic phase: Identification and management: Clin Lymphoma Myeloma Leuk, 2017; 17(2); 78-82
14.. Heffner J, Etiology, Clinical presentation, and diagnosis of chylothorax UpToDate May 2022 [cited 2022 Oct 4]. Available from: [Subscription required]https://www.uptodate.com/contents/etiology-clinical-presentation-and-diagnosis-of-chylothorax?search=chylothorax&source=search_result&selectedTitle=1~74&usage_type=default&display_rank=1#H6
15.. Sammartino D, Khanijo S, Koenig S, Chylothorax in patients with chronic lymphocytic leukemia: A case series: J Hematol, 2018; 7(1); 14-18
16.. Rice TW, Milstone AP, Chylothorax as a result of chronic lymphocytic leukemia: Case report and review of the literature: South Med J, 2004; 97(3); 291-94
17.. McGrath EE, Blades Z, Anderson PB, Chylothorax: Aetiology, diagnosis and therapeutic options: Respir Med, 2010; 104(1); 1-8
18.. Koylu B, Tekin F, Aktas BY, Pazopanib-induced chylothorax in a patient with renal cell carcinoma: Anticancer Drugs, 2022; 33(1); e555-e57
19.. Phan C, Jutant EM, Tu L, Dasatinib increases endothelial permeability leading to pleural effusion: Eur Respir J, 2018; 51(1); 1701096
20.. Van Renterghem DM, Pauwels RA, Chylothorax and pleural effusion as late complications of thoracic irradiation: Chest, 1995; 108(3); 886-87
Tables
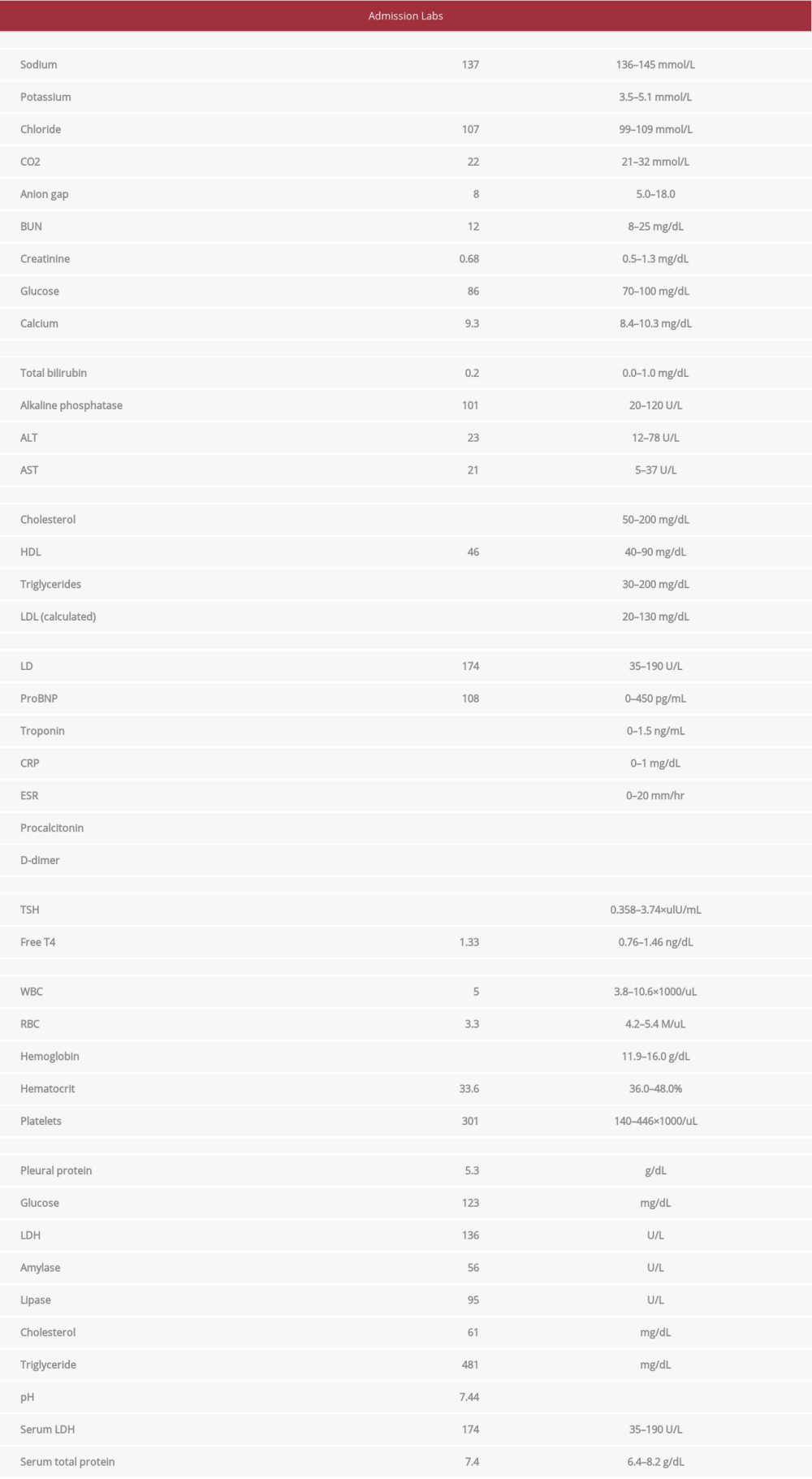 Table 1.. Admission laboratory findings and pleural fluid analysis.
Table 1.. Admission laboratory findings and pleural fluid analysis.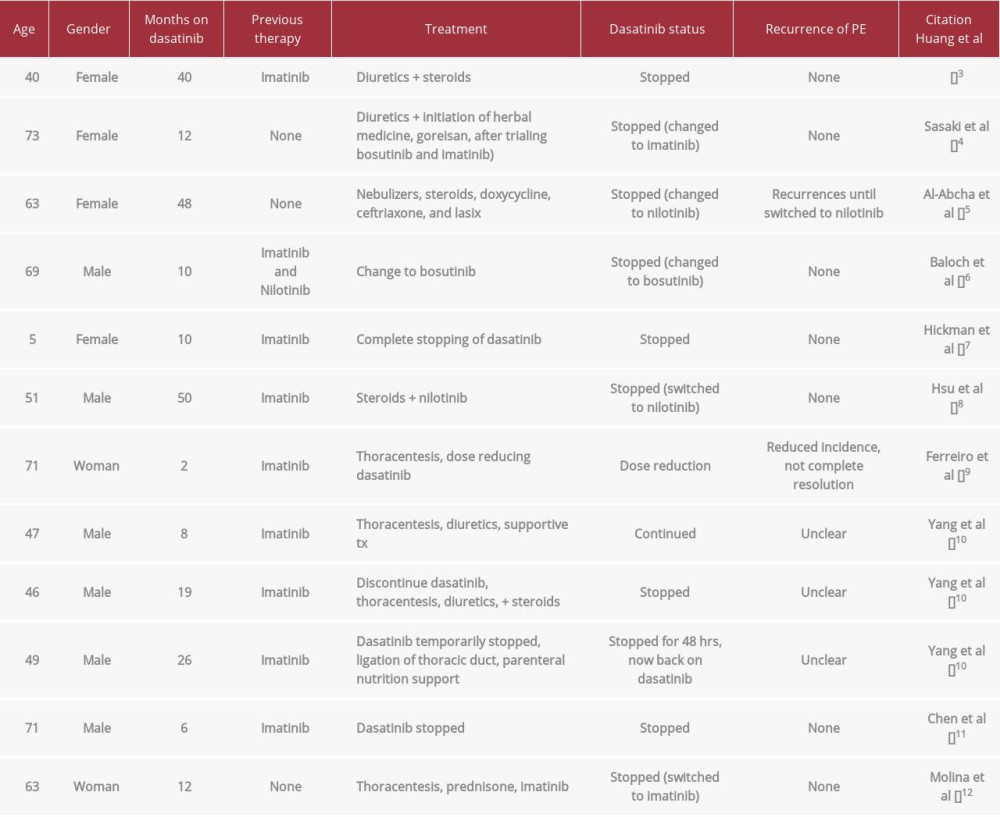 Table 2.. Review of cases associated with Dasatinib-induced chylothorax and outcomes.Table 1.. Admission laboratory findings and pleural fluid analysis.Table 2.. Review of cases associated with Dasatinib-induced chylothorax and outcomes.
Table 2.. Review of cases associated with Dasatinib-induced chylothorax and outcomes.Table 1.. Admission laboratory findings and pleural fluid analysis.Table 2.. Review of cases associated with Dasatinib-induced chylothorax and outcomes. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133